Download
1 / 46
470 likes | 504 Views
Explore the potential of HIV vaccines to control the epidemic, current vaccine strategies in development, and the importance of targeting mother-to-child transmission. Discover the latest clinical advancements and challenges in scaling up vaccine deployment for maximum impact.

E N D
The role of HIV vaccines in achieving HIV epidemic control Glenda Gray President & CEO SAMRC HVTN Co-Principal Investigator Achieving HIV Control IAS 2019, Mexico City, Mexico, 22nd July 2019
UNAIDS has declared that a 90% reduction in incidence from 2010 in each country would end the aids epidemic as a public health threat
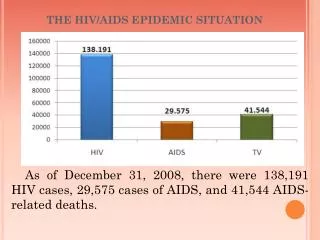
EPIDEMIC CONTROL: <1/10 000 per year Concordant with WHO definition to define control for other diseases. Temporal Milestones: 1/1000 by 2030 1/10 000 by 2035 RSA: 11.5/1000 (2018) RSA: 1/1000 in 2030=91.3% drop
Could an HIV vaccine truly control the epidemic? • What vaccine strategies are in advanced clinical development that could be deployed ? • Could we use a vaccine to eliminate mother to child transmission of HIV? • How to scale-up deployment for maximum benefit?
But OUR HIV EPIDEMIC IS NOT UNDER CONTROL.OUR INTERVENTIONS ARE NOT enough to meet global targets Source: UNAIDS 2019
IN THE HARDEST HIT COUNTRY, South Africa WE ARE WAY off our 90:90:90 aspirations UNAIDS DATA 2019
We are hopelessly off track to meet the target 0.1% by 2030 Personal Communication: Debbie Bradshaw & Rob Dorrington
That’s why we need something that is disruptive: HIV Vaccine
CURRENT HVTN APPROACHES IN THE CLINIC 3. Active Immunization to induce neutralizing antibodies (POC) 1. Active Immunization to induce binding antibodies 2. Passive Immunization (POC) Coaxing the immune system to develop broadly neutralizing antibodies with immunogens e.g. lineage based vaccine design, germline targeting or epitope based vaccine design. Vaccination to stimulate binding antibodies previously shown to correlate with reduced risk of HIV infection in RV144 or in NHP challenge models. This is being tested in the large efficacy trials: HVTN 702, HVTN 705, HVTN 706 Pre-formed broadly neutralizing antibody e.g. VRC 01, a neutralizing antibody targeting the CD4 binding site. This is being tested in the HVTN POC 703 (AMP trial). Other NABs targeting other sites on the env are being evaluated in phase 1. Adapted from a slide from Lynn Morris
Current NIH/HVTN HIV Vaccine Strategies HVTN702: Phase 2b/3 Clade C ALVAC + gp120 in MF59 Empirical Vaccines to improve potency and durability of non-neutralizing anti-Env V2 Abs HVTN705: Phase 2b Mosaic Ad26 + Clade C gp140 RV144 Thai Trial HVTN706: Phase 3 Mosaic Ad26+Clade C gp140 and Mosaic gp140 Phase 1/2a: Alternative Viral Vectors and Env Proteins Theoretical Vaccines that induce bNAbs Phase 1: rENV Immunogens for bNAbs, alternative adjuvants PMTCT Broadly Neutralizing Antibodies Immunoprophylaxis with bNAbs Mab cocktails HVTN703/704: Phase 2b AMP Trials VRC01 mAb Source: Slide adapted from Mary Marovich, NIH & J. McElrath HVTN
The rationale for advancing these candidates into efficacy trials 5407 fully enrolled 1900 fully enrolled 2637 fully enrolled 3800 to be enrolled
WE ARE WORKING HARD TO ACHIEVE THESE NUMBERS Ndola Mbeya Kisumu Maputo Lilongwe Elandsdoorn Lilongwe Mamelodi Blantyre Soshanguve Lusaka (2) Medunsa Harare (2) Harare (2) Johannesburg Gaborone Ladysmith Tembisa (2) Soweto (2) Rustenburg Vulindlela HVTN NETWORK SITES Groote Schuur Durban (6) HPTN SITES Klerksdorp Bloemfontein PROTOCOL-SPECIFIC SITES Cape Town (4) Mthatha These are the trailblazers in this heroic endevour
RATIONALE FOR HVTN 702 IS BASED ON RV144 Correlates associated with ↓HIV acquisition: • Abs (IgG, IgG3) against envelope (vaccine-matched gp120, V1V2) • Functionality, polyfunctionality scores of env-specific CD4+ T-cell responses V1V2 loop V3 loop • Vaccine efficacy wanes • magnitude, quality and durability of immune responses wanes Rerks-Ngarm S. et al. N. Engl. J. Med. 2009; Corey L et al. Science Transl. Med. 2015. Haynes BF Courtesy: Fatima Laher
HVTN 702 572 site research staff 14 trial sites in South Africa 5407 enrolled by june 2019 >100 000 PBMCs thusfar
RATIONALE FOR HVTN 705: The Ad26/Ad26+Env HIV vaccine regimen provides substantial protection against SHIVSF162P3 challenges in non-human primates [study designed to mimic APPROACH trial (HIV-V-A004)] 6x IR SHIV challenges prime prime boost boost 0 6 12 18 months 3 N = 12 per group
RATIONALE FOR HVTN 705/HPX2008: Vaccine Aiming at Protection Against all Clades ofHIV-1 Adolescents(11-17 years) /Adults(18-65 years) in endemic countries and populations at risk in Western world Different HIV-1 clades dominate in different geographicregions 3 Trimeric env protein for improved humoral immunity 1 Potent primingVectors 2 Mosaic insertsfor globalcoverage Low seroprevalentAd26 Ad26.HIV-Gag-Pol Ad26.HIV-Env (MVA.HIV-Gag-Pol-Env) Dan H Barouch et al.,2010 19
Mixture of 4 mosaic Ad26 constructs + gp140 Clade C boost Boost Prime gp140 Clade C Soluble trimer gp140 env proteins Ad26.Mos4.HIV gag-pol-env Ad26.Mos4.HIV gag-pol-env + Ad26.Mos4.HIV Ad26 vectors with Mosaic gag-pol or env inserts Ad26.Mos1.Gag-Pol Ad26.Mos2.Gag-Pol Ad26.Mos1.Env Ad26.Mos2S.Env (clade B-like) (clade C-like) prime prime boost boost 0 6 12 months 3
Multi-center Phase 3 Efficacy Study GLOBAL SITE DISTRIBUTION AMERICAS UNITED STATES of AMERICA = 24 sites (11 pending) Sites in TX, FL, GA, LA, IL, DC, TN, NJ, NY, MA,PA, OH, WA, CA EUROPE POLAND = 3 sites Sites in Warsaw, Gdansk, Wroclaw MEXICO = 3 sites Sites in DF, Merida and Guadalajara BRAZIL = 8 sites Sites in Rio, Belo Horizonte, Sao Paolo, Curitiba, Salvador and Manaos PERU = 5 sites Sites in Lima and Iquitos SPAIN = 6 sites Sites In Madrid, Barcelona, Valencia and Cordoba ITALY = 3 sites Sites in Milan, Roma and Modena ARGENTINA = 3 sites Sites in Buenos Aires and Rosario
HPX3002/HVTN706/MOSAICO: Study Overview • 3,800 participants; randomized in a 1:1 ratio to the study vaccine or placebo (randomization will be stratified by site) Vaccine Primary Analysis 1:1 randomization N=3800 N=1900 Go/no-Go Roll over study to further assess durability Placebo N=1900 • Follow‑up: • At least 24 months after the 3rd vaccination in participants who remain HIV‑1 negative • 6 months after diagnosis of HIV-1 infection in participants who become HIV-1 infected Mo. 24-30 1.5-2 years after Vac 3 # Ad26.Mos4.HIV=5x1010vp *Clade C + Mosaic gp140= 125 + 125 micrograms of glycoprotein 22
Rationale for AMP Study: potency of VRC01 In VitroNeutralization (IC80) % of viruses resistant to neutralization, IC80 > 50µg/ml 45% 21% 12% 5% 36% 3% • Neutralizes 80%-90% of viruses (all major clades) • Mean IC80 = 1.0 ug/ml; potential to work at physiologically attainable levels. Panel of 170 genetically diverse Env-pseudoviruses, representing all major clades Line shows median IC value - based on results from all viruses, including those not neutralized.
RATIONALE FOR AMP STUDY: VRC01 Protects Against Mucosal SHIV-Challenge in Non-Human Primates 20 mg/kg infusion of VRC01: Challenge with SHIV SF162P3 VAGINAL CHALLENGE RECTAL CHALLENGE 4/4 protected 4/4 protected 0/4 protected 1/4 protected • Pegu et al. Science Transl Med (2014) • Ko et al. Nature (2014) • Rudicell et al. J Virol (2014)
Cohorts for the AMPStudies * Due to the randomization scheme, the numbers of vaccine and control recipients may differ slightly.
AMP Study Research Sites HVTN 704/HPTN 085,MSM + TG HVTN 703/HPTN 081,Women
USING Antibody-based Vaccine Design for PMTCT Start with a known human bNAb V1V2 Glycan Glycans Glycan-V3 Supersite • Design a vaccine to elicit a similar neutralizing antibody CD4 binding site gp120-gp41 Interface Membrane-proximal external region (MPER) Viral membrane Image by Stewart-Jones, Doria-Rose, Stuckey Adapted from Stewart-Jones et al Cell 2016 and Pancera et al Nature 2014 Slide Adapted Courtesy of J. Mascola
Can a vaccine can eliminate breastmilk transmission? Stagnating rates of PMTCT Ameena Goga, et al SAMRC
INFANTS MAKE MORE Nabs quicker & with less somatic hypermutation • HIV infected infants produce more neutralizing antibodies than binding antibodies • More likely to develop neutralization breadth earlier
HVTN 135: evaluating the role of CH505TF gp120 to induce NAB in infants exposed to HIV CH505TF gp120 was derived from a clade C transmitted/founder virus isolated from an acute-seroconversion sample, selected based on its binding affinity to the CH103 bnAb lineage.
HIV vaccine impact on new infections: Brazil No Vaccine Adolescents MSM, IDU, Mid- high risk heterosexual 15-49 years Fonseca MGP, Forsythe S, Menezes A, Vuthoori S, Possas C, et al. (2010) Modeling HIV Vaccines in Brazil: Assessing the Impact of a Future HIV Vaccine on Reducing New Infections, Mortality and Number of People Receiving ARV. PLOS ONE 5(7): e11736. https://doi.org/10.1371/journal.pone.0011736 https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0011736
IMPACT OF HIV VACINATION IN CHINA Number of new adult infections in Sichuan Province Harmon T, Schwartlander B, Vaccines, 2015
Modelling P5-hvtn 702 regimen IN RSA Cumulative VE Boosters Selinger C, Gray G, et al. Vaccines, 2019
The impact of targeting & durability: Fast track WITH prep versus status QUO (ART roll-out) without prep Selinger C, Gray G, et al Vaccines, 2019
TARGETING SCENARIOS Attrition 0% 20% 50% Selinger C, Gray G, et al. Vaccines, 2019
How to go to scale: my 10 cents worth • Cohort vaccination in RSA at 50-80% coverage: 6-9 million vaccine regimens over 20 years • To be cost-effective $176-$354 • Immunization supply chain: effective vaccine management practices, system redesign with sub-district strengthening • TARGETED APPROACH TO INCREASE PUBLIC HEALTH BENEFIT
Summary • The products in advanced clinical development may be the first generation HIV vaccines that go into the clinic • If any of the vaccines or antibodies are effective it will unleash an enormous explosion in scientific inquiry to improve, adapt and most importantly bring to the world a new form of HIV prevention • An HIV vaccine will be the most complex vaccine ever designed but the science is exciting and novel
Humans must be clever to conquer a clever adversary but with persistence we can and will beat this sucker. (Larry Corey)
All the study staff, the community engagement teams, and most of all, the participants who join the journey ACKNOWLEDGEMENTS
Acknowledgments HVTN Core, SDMC, EMT Larry Corey (HVTN PI), Peter Gilbert, Jim Kublin, Susan Buchbinder, Scott Hammer, Dan Barouch Shelly Karuna, Jacky Odhiambo Avy Violari &HVTN 135 Team HPTN Mike Cohen,Srilatha Edupuganti, Nyaradzo Mgodi HVTN Lab Program Julie McElrath, Georgia Tomaras, John Hural, David Montefiori, Steve DeRosa, Erica Andersen-Nissen, Guido Ferrari CHAVI ID Bart Haynes, Larry Liao and colleagues DAIDS Vaccine Research Program Carl Dieffenbach, Mary Marovich, Dale Hu, Phil Renzullo, Pat D’Souza, Paul Kitsutani, Mary Allen, Jim Lane, Mike Pensiero VRC John Mascola & Team SAMRC Ameena Goga Michelle Mulder DST Glaudina Loots
Collaborators - Africa • Fatima Laher • Erica Lazarus • Linda Gail-Bekker • Gita Ramjee • Cheryl Louw • Pam Mda • Kathy Mngadi • Graeme Meintjes • Craig Innes • Phillip Kotze • Francis Martinson • Jani Ilesh • Stewart Reid • Leonard Maboko • MaphoshaneNchabeleng • LungiswaMtingi • DumezweniNtshangase • William Brumskine • ZvavaheraChirenje • MookhoMalahlela • ModulakgotlaSebe
NIAID/DAIDS Acknowledgements NIAID/DAIDS Senior Management Anthony S. Fauci Carl Dieffenbach Preclinical Research Development Branch Jim Bradac (Branch Chief) Que Dang Angela Malaspina Nancy Miller Jessica Santos Alan Schultz Stuart Shapiro Anjali Singh Jonathan Warren Vaccine Translational Research Branch Michael Pensiero (Branch Chief) • Maria Chiuchiolo • Jennifer Grossman • Christopher Hamlin • Sonia Gales • Vijay Mehra • Ruchi Raval • Shah Raza • Shyam Rele • Nandini Sane • Amanda Ulloa • Sujata Vijh VRP- Office of the Director Kevin Ryan Barbara Cunningham Sherolyn Earle Mary Nguyen Tina Tong Vaccine Clinical Research Branch Dale Hu (Branch Chief) Philip Renzullo Mary Allen Jane Baumblatt Cesar Boggiano Maggie Brewinski-Isaacs Patricia D’Souza Margarita Gomez Julia Hutter Nina Kunwar James Lane Pierre Paisible Laura Polakowski Edith Swann NIAID funded Networks and Partners VRC: John Mascola, Julie Ledgerwood, Barney Graham, Rick Koup Janssen: Maria Pau, Frank Tomaka Pox Protein Public Private Partnership (P5):