Download
1 / 18
180 likes | 195 Views
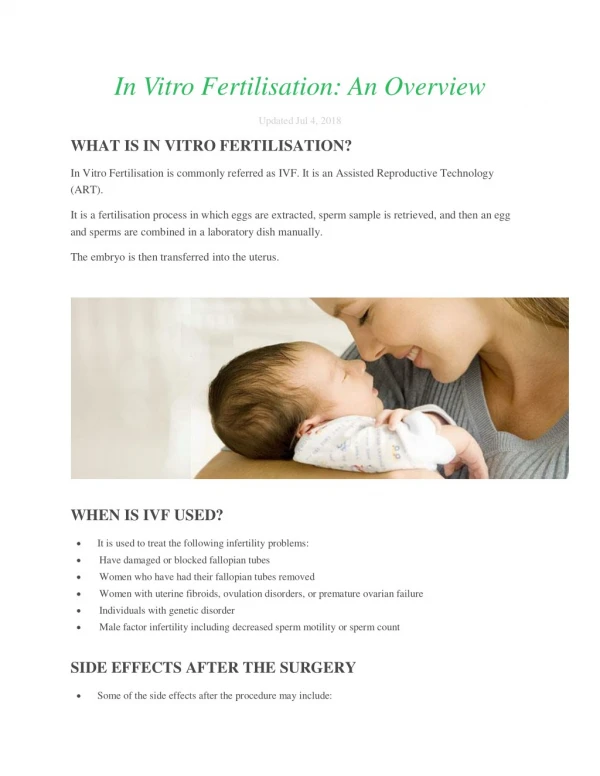
Explore the complexity of in vitro fertilization (IVF) treatment for heterosexual couples in the realms of health law and bioethics, including assisted reproductive technologies, donor options, and the history of IVF.

E N D
Problems with the In Vitro Fertilisation Treatment of Heterosexual Couples Health Law and Bioethics Georgi Avramov, Student Number: 004794, Erasmus + Student from Sofia University “St. KlimentOhridsky”
What Is Inferitily? • One possible definition: infertility is the failure to conceive after a specific period of time of regular, unprotected sexual intercourse, or the occurrence of three or more consecutive miscarriages or stillbirths. • Specific period of time: • standard definition – 12 months; • World Health Organisation (WHO) – 2 years; • some demographers – 5 years. (Image source: http://portugalresident.com/facing-and-treating-infertility) • Actual incidence of fertility problems – unknowable; now assumed - one in six heterosexual couples.
What are assisted reproductive technologies? • Assisted reproductive technology (ART) is the use of reproductive technology to treat infertility. Examples include in vitro fertilization (IVF) and its possible expansions, such as: • cryopreservation of sperm, oocytes, embryos; • artificial insemination; • in vitro generated gametes; • IVF; • cloning etc.
1. Cryopreservation (Image source: http://sites.davidson.edu/bio362_art/?page_id=38) • What is Cryopreservation? Freezing of: • sperm (first frozen 1949); • embryos (first frozen 1983); • eggs (until recently considered as unsafe procedure, now possible).
2. Assisted Insemination by Husband/Partner (AIH/AIP) • It is the assisted insemination with sperm of the husband or the partner. • No longer the optimum treatment for men with poor quality sperm. • Continues to be used in case of treatments such as chemotherapy, that will render the man infertile.
3. Donor Insemination (DI) • 1st recorded DI – end of the 19thcentury. • Disapproved and not acceptable until recently. • Common reasons – partner’s infertility, genetic disease, sexual dysfunction. • DI – still the only chance in cases of a man, who could not produce any sperm, or a woman without a partner. • Low success rates. (Image source: http://ivfmohali.com/our-services/donor-insemination-d-i/)
4. Oocyte (Egg) Donation (Image source: http://www.simpledonations.com/egg-donors/) • Important differences from DI: • Finite number of eggs; • Much more uncomfortable and invasive; • First used in IVF treatment in 1984; • The freezing of eggs is also in infancy compared to the freezing of sperm; • Some countries prohibit it. • Common reasons - ovarian failure, a serious genetic abnormality; also multiple failed IVF treatment with own eggs. • Procedure – like the IVF treatment. • Advantage – biological connection to the child, always a legal mother of the child.
5. Gamete Intra-Fallopian Transfer (GIFT) • In Vivo - egg retrieval in the same way as IVF, but instead of being placed in a petri dish with the sperm, the eggs and the sperm are injected into the woman’s fallopian tube. • Common reasons - no abnormality in a woman’s fallopian tubes and the couple’s infertility is “unexplained”. (Image source: http://lakecharlesobgyn.com/Complete/397-GIFT.aspx)
6. Micromanipulation: Intra-Cytoplasmic Injection (ICSI) and Sub-Zonal Insemination (SUZI) • ICSI: • injection of a single sperm into an egg with a very fine glass needle; • if fertilisation occurs - zygote(s) will be transferred to the women’s uterus in the same way as in conventional IVF; • common reasons - sperm cannot penetrate an egg naturally (extremely low sperm count or poor motility). • SUZI: • microinjection of a small number of sperm into the egg; • it might be used if normal fertilisation has failed to occur. • Success rates improved dramatically over the years.
7. Cloning • Dolly the sheep – 1997. • In theory could be used to increase the numbers of embryos created in an IVF cycle, or to create a duplicate embryo that could be tested for genetic abnormailities and discarded, while its intact “twin” could subsequently be implanted. (Image source: http://usatoday30.usatoday.com/tech/science/genetics/2006-07-04-dolly-anniversary_x.htm)
(8.) In Vitro Fertilisation (IVF) History: • Research began in the 1930s. • 1st successfully performed on mouse in 1958. • IVF with human gametes - pioneered by Robert Edwards and Patrick Steptoe during the 1960s and 1970s -> first IVF baby, Louise Brown (25.07.1978). • Initially - hostility to IVF and scepticism about its safety and efficacy. (Imagesource: http://www.dailymail.co.uk/news/article-2515585/Louise-Brown-Worlds-test-tube-baby-pays-emotional-tribute-parents.html) (Imagesource: http://www.dailymail.co.uk/health/article-3173446/World-s-test-tube-baby-reveals-mother-received-blood-splattered-HATE-MAIL-born-including-letter-containing-plastic-foetus.html)
In Vitro Fertilisation (IVF) (Imagesource: http://www.mexicalihealthcare.com/procedure/In-Vitro-Fertilization/21) Procedure: 1. Commonly hormonal treatment – producing more eggs. 2. Removal of the eggs from the ovarian follicles through laparoscopy or transvaginal aspiration and placing them in a culture that allows them to mature further. 3. Providing of sperm. 4. Putting the mature eggs into a petri dish with sperm (usually from the woman’s partner). 5. If fertilisation occurs the resulting zygote(s) may be places in the woman’s uterus, or frozen to be used at a later date.
In Vitro Fertilisation (IVF) Nowadays: • IVF is now the most common treatment for infertility (99 % of all procedures). • Success rates - depend on a number of factors. The most recent report from 2009 found: • Pregnancy achieved - 29.4% of all cycles (higher or lower depending on the age of the woman); • Live births - 22.4% on average (higher or lower depending on the age of the woman). • More than 5 million babies have been born in the world as a result of an IVF treatment.
The Steinkamp Family (in 2008) (Image source: http://www.kinderwunsch-nrw.de/templates/media/pdf/SpiegelDokumente-25_05_2008.pdf)
Problems with IVF Treatment • Unnaturalness • Child welfare • Ignoring Infertile Women • Equality • Low success rates • Multiple pregnancies • Informed decision – not informed enough • Infertility treatment “takes over” patient’s lives • Extremely expensive
What and How Should We Regulate? • Access to treatment • Consultation and informed consente • Status and Use of Gametes • Status and Use of Gametes • Procedure • Paternity • Regulating new technologies