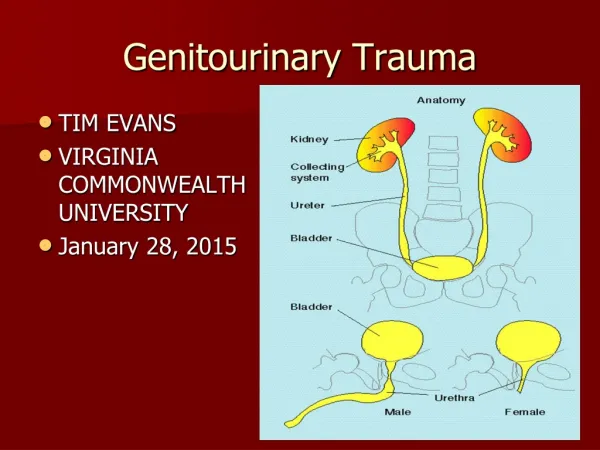
Genitourinary
Genitourinary. Common Genitourinary Disorders. Enuresis Urinary Tract Infection Pyelonephritis Vesicoureteral reflux (VUR) Hydronephrosis Cryptorchidism Hypospadius Exstrophy of Bladder Acute Glomerulonephritis Nephrotic Syndrome Acute Renal Failure. Voiding. Toilet Training.


Genitourinary
E N D
Presentation Transcript
Common Genitourinary Disorders • Enuresis • Urinary Tract Infection • Pyelonephritis • Vesicoureteral reflux (VUR) • Hydronephrosis • Cryptorchidism • Hypospadius • Exstrophy of Bladder • Acute Glomerulonephritis • Nephrotic Syndrome • Acute Renal Failure
Toilet Training • Myelination of spinal cord necessary before child can control bowel and bladder function; occurs between 12-18 months • However, child is usually not ready until 18-24 months • Waiting until 24-30 months makes the job easier
Toilet Training: Average age of Continence is 3 years of age Expected Developmental Milestones
Signs of Readiness for Toilet Training • Physical Readiness • Child removes own clothes • Child is willing to let go of toy • Child is able to sit, squat, and walk well • Child has been walking for 1 year • Psychological Readiness • Child notices wet diaper • Child indicates need for diaper change • Child communicates need to go to the bathroom and can get there by self • Child wants to stay dry
Parent Readiness • Requires many toileting sessions a day • Need to be able to give child undivided attention • Patience • Personal choice on toilet or free standing potty chair
EnuresisInvoluntary voiding of urine > 6 yrs • Primary • Never achieved dryness for 3 months • Secondary • Dry for 3-6 months then resumes wetness • Diurnal • Wetting occurs only in daytime • Nocturnal • Wetting occurs only in nightime
Etiology Organic • Neurological delay • UTI • Structural disorder • Chronic renal failure • Disease with polyuria (DM) • Chronic constipation
Etiology Non-organic • Sleep arousal problem • Sleep disorders from enlarged tonsils, sleep apnea • Psychological stress • Family history • Inappropriate toilet training
Diagnosis • Physical exam to r/o organic cause • Made by voiding diary
Treatment • Organic- treat underlying cause • Nonorganic- most will outgrow by late childhood
Impact on child • May avoid activities • Sports • Sleepovers • Great source of stress • Concealing wet clothing is difficult • Odor is a concern
Enuresis: Nursing Diagnosis • Situational Low Self-Esteem related to bed- wetting or urinary incontinence • Impaired Social Interaction related to bed- wetting or urinary incontinence • Compromised Family Coping related to negative social stigma and increased laundry load • Risk for Impaired Skin Integrity related to prolonged contact with urine
Assess parent and child’s motivation and readiness • If willing to be active participant then management includes: • Alarms • Timed voiding • Bladder exercises • Elimination diets • Behavioral therapy • Medications
Medication • DDAVP • Ditropan • Tofranil (Imipramine)
Urinary Tract Infection(UTI) • Most common infection of GI tract • Fecal bacteria (E. coli) cause most UTI’s • Girls>boys after age 1 • In males uncircumcised>circumcised • Can lead to renal scarring, high blood pressure, End Stage Renal Disease
Conditions that Predispose Infants and Children to UTIs • Urinary tract obstructions • Voiding dysfunction resulting in urinary stasis • Anatomic differences in younger children • Individual susceptibility to infection • Urinary retention while toilet-training • Bacterial colonization of the prepuce of uncircumcised infants • Infrequent voiding • Sexually active adolescent girls
Symptoms • Infants • Nonspecific • Fever or hypothermia (neonate) • Irritability • Dysuria (crying when voiding) • Change in urine odor or color • Poor weight gain • Feeding difficulties
Symptoms • Children • Abdominal or suprapubic pain • Voiding frequency • Voiding urgency • Dysuria • New or increased incidence of enuresis • Fever • Malodorus urine • Hematuria
Pyelonephritis Infection travels to kidneys Symptoms • Same s/s of UTI plus: • Higher fever • Back or flank pain (CVAT) • Nausea & vomiting • Look sick
Diagnostic tests • Urinealysis (UA) • Macro • Micro • 24 hour • Culture and Sensitivity (C & S) • Specimen collection • Clean catch • Pediatric urine collector • Straight cath • Foley cath
Diagnosis • UA (Urinalysis) • Bacteriuria • Pyuria • Urine C&S: colony count = 100,000 • Pyelonephritis • Above plus • Elevated WBC • Elevated ESR • Increased CRP
Management of Both • 7-10 day course of ABX • Dehydrated child and very young often require IV and hosp • Increase PO fluids • Analgesia • Antipyretics • Repeat urine C&S 3-5 days after tx
Prevention • Proper toilet training • Teach proper wiping • Avoid tight clothing • Wear cotton underwear • Encourage children to avoid “holding” urine • Avoid bubble baths • Don’t force cranberry-increases acidity • Adolescent: urinate immediately after intercourse
Vesicoureteral reflux (VUR) • Malformed valves at ureters and bladder • Allows a backflow of urine up the ureter into the kidney • Can be congenital abnormality, graded 1-5 • Grade 5: massive ureteral and renal pelvis dilation
Etiology and symptoms • Genetic origin • Girls>boys • Symptoms • Frequent UTI’s (most common) • Enuresis • Flank pain • Abdominal pain
Vesicoureteral reflux (VUR) Treatment: • Grades 1-3: will usually resolve on own • Grades 4-5: valve repair • Prophylactic ABX • Teach child to double void • Urine C&S q 2-4 months until 3 negative
Hydronephrosis • Enlargement of the pelvis of the kidney secondary to a congenital narrowing of the ureteropelvic junction • May also be acquired secondary to kidney stones, tumors, blood clots
Symptoms • Usually free of symptoms initially • May have repeated UTI’s (urinary stasis) • Polyuria • Frequency • Flank pain • Increased BP • Abdominal palpation reveals a mass
Hydronephrosis Diagnosis: • If congenital, usually diagnosed in utero • IVP shows enlarged renal pelvis & site of obstruction Management: • If untreated can destroy nephrons • Surgical correction of the obstruction
Cryptorchidism (UDT) • One or both testes fail to descend through the inguinal canal into the scrotal sac • Testis may be retractable • In 85% right testis is affected • The affected side or bilateral scrotum appears flaccid or smaller than normal • Unknown why this fails • Increased abd pressure • Hormonal influences
Cryptorchidism (UDT) • Common in the premature infant and LBW infant • Incidence decreases with age • Many resolve spontaneously by 12 months age • If still present at age 1, descent usually does not occur • Associated with lower sperm production • Increased risk for malignant testicle turoms in adulthood
Management • Observation for first year • HCG- stimulates testosterone production and helps with descent • If testis fail to descend between 1-2 years of age then surgical treatment: Orchiopexy
Surgical Management: usually outpatient • Post op instructions: • Loose clothing • Incision Care • Monitor for infection • Analgesia • Ice • Discuss future fertility & cancer risk
Hypospadius • Congenital malformation • Urethral opening is below normal placement on glans of penis (ventral surface-underside) • May also have short chordee (fibrous band of the penis, will cause it to curve downward) Epispadius • dorsal placement of urethral opening
Etiology and Symptoms • Cause is unknown • Defects in testosterone is possible • Possible genetic origin Symptoms • Urinary stream deflected downward • Prepuce is small-Penis appears to look circumcised • May have chordee, undescended testes and inguinal hernia
Management of both • Out patient surgery to lengthens urethra (meatomy), position meatus at penile tip, release the chordee • Performed btw 12-18 mos of age • No circumcision
Post-op: • Stent for urinary drainage and patency • Double Diapering • Strict I&O • Pain Management • Monitor for Infection • No Hip-Holding, ride-on toys • Possible fertility problems
Exstrophy of Bladder • Bladder lies open and exposed on abdomen (defect in abdominal wall) • Pelvic bone defects (non-closure of pelvic arch) • Bladder is bright red & unable to contain urine, may also have defects in urethra (epispadius) • Surgical closure of abdominal wall, reconstruction of bladder, urethra and genitalia “continent urinary reservoir”
Management Preop: Prevent infection Protect skin integrity Protect exposed bladder Parental education (straight catheterization) Keep infant’s legs flexed
Goals of Surgery • Closure of the bladder and abdominal wall • Urinary continence, with preservation of renal function • Creation of functional and normal-appearing genitalia • Correction to promote later sexual functioning
Post Op • Suprapubic catheter-if unable to restore function • Immobilized Pelvis • Strict I&O • Antispasmotics: Probanthine (Pyridium) • Analgesics • Parental Emotional Support
Summary-Nursing Role Structural Disorders of GU System • Many children are discharged with stents or catheters. • Teach parents how to change dressings, double diaper, care for catheters, assess pain and give analgesics, and recognize signs of possible obstruction or infection. • Parents should encourage the child to participate in age-appropriate activities.
Pediatric Normal Value age 2-12 yr • Chemistry Panel • Potassium: 3.5-5.8 • Sodium: 135-148 • Urea Nitrogen: 3.5-7.1 • Creatinine: 0.2-0.9 • Calcium: 2.2-2.7 • Albumin: 3.2-4.7 • Blood Gases • Bicarbonate: 18-25 • Urinalysis • Protein: None • Specific Gravity: 1.001-1.030
Acute Glomerulonephritis (AGN) • Sudden inflammation of the glomeruli of the kidney resulting in acute renal failure • Peak age 5-10 years, boys>girls • Capillary walls of kidney become permeable; allows red blood cells and protein to pass into urine • Usually seen 7-10 days after a strep infection (immune response to strep), may be other organisism • APSGN (Acute Post Streptococcal Glomerulonephritis)