Download
1 / 31
400 likes | 849 Views
CELIAC DISEASE. A Lifetime Without Beer. Kyle Mulligan Northwestern Ontario Medical Program. Outline. Epidemiology Pathogenesis Clinical Features Associated Conditions Diagnosis Treatment. Epidemiology. True prevalence unknown Variable symptoms Slight female preponderance

E N D
CELIAC DISEASE A Lifetime Without Beer Kyle Mulligan Northwestern Ontario Medical Program
Outline • Epidemiology • Pathogenesis • Clinical Features • Associated Conditions • Diagnosis • Treatment
Epidemiology • True prevalence unknown • Variable symptoms • Slight female preponderance • Highest prevalence in Western Europe and emigrants (North America, Australia) • Also India, South America, North Africa • Low African-Caribbean, Chinese, Japanese
Prevalence Studies • One case in every 300 newborns • 1 in 266 prevalence for asymptomatic cases in blood donors • In the USA, elevated antiendomysial antibodies in 1:250 healthy blood donors Relatively common and Underdiagnosed.
Pathogenesis • Immune system abnormally activated by gluten • Gliadin portion of wheat protein • Prolamines (insoluble proteins) in rye, barley and oats
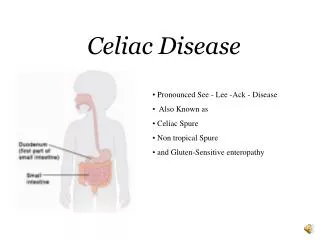
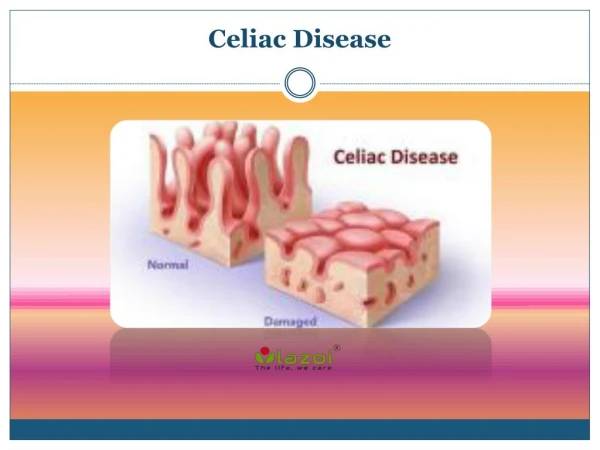
Pathogenesis • Genetic, immunologically-mediated, small intestine enteropathy in which intestinal villi are destroyed by cellular and humoral-mediated immunologic reaction to gliadin protein • Results in malabsorption
Pathogenesis • Inappropriate T-cell mediated immune response in genetically predisposed people • 10% prevalence among 1st degree relatives • 95% express HLA-DQ which presents gluten-derived gliadin peptides to stimulate T-cells • Delaying exposure to gluten may alter disease
Pathogenesis • Viral exposures may trigger an immunologic response • Adenovirus type 12 implicated • Enzyme tissue transglutaminase is one of the targets of the autoimmune response in celiac disease
CLINICAL: Classical children • Present btwn 4-24m with impaired growth, FTT, diarrhea, and abdominal distension • Vomiting common, pallor, edema • Gradual onset • Wt gain velocity slows then wt loss • Severe: growth delays, iron and folate deficiency anemia, rickets, pubertal delay
CLINICAL: Atypical children • Older child and adolescents • Recurrent abdominal pain, transaminases, recurrent aphthous stomatitis, defects in dental enamel, angular cheilitis • Arthralgia • Depression, irritability, poor school performance • Atopic dermatitis
CLINICAL: adults • 20% of cases occur in people >60 yo • May present in pregnancy and post-partum as anemia • Episodic or nocturnal diarrhea, flatulence, and weight loss • Symptomatic lactose intolerance because of the enteropathy
CLINICAL: adults • Steatorrhea often absent especially if disease proximal small intestine • Abdominal discomfort and bloating common and may be Dx as IBS • Malaise and “tired all the time” very common • Consider with stomatitis, angular cheilitis
CLINICAL: adults • Only 50% with diarrhea • Most common presentation is Fe deficiency
Extra-Intestinal Manifestations • Nutritional deficiencies: • Iron deficiency anemia • Folate/B12 (anemia, glossitis, peripheral neuropathy, • Vitamin K (coagulopathy, purpura) • Vitamin D which can lead to hypocalcemia/tetany, elevated ALP, and osteoporosis • Protein (edema, ascites) • Vitamin A (night blindness)
Associated Conditions • Dermatitis Herpetiformis • Intensely pruritic papulovesicular lesions occurring symmetrically over extensor surfaces, buttocks, trunk, neck, and scalp • Responds to gluten free diet • Diabetes Mellitus type I • ~8% positive rate in asymptomatic DM I children • Autoimmune Thyroiditis
Associated Conditions • Seizure Disorder • Occipital calcification • IgA nephropathy • IgA deficiency • Sjogren’s syndrome/ Rheumatoid Arthritis/ Collagen Disorders • Down’s Syndrome
Diagnosis • One study showed that a subset of patients with adult-onset celiac disease had symptoms and were followed by a physician for 28 years before Dx • 43% of Canadian celiac disease patients misdiagnosed previously (IBS, stress, anemia, colitis, food allergy, PUD)
Diagnosis • Routine tests that can suggest celiac disease • Anemia (microcytic, hypochromic or normocytic, normochromic with RDW) • AST • Albumin/plasma protein • Low or “too good” cholesterol (total, LDL, HDL) • alkaline phosphatase
Diagnosis • Currently, Ontario laboratories screen with IgA antiendomysial antibody and tissue transglutimase antibody • If positive other tests can be ordered • MDS charges, in hospital does not • May want to test for IgA deficiency before writing off a false test
Diagnosis • Presence of IgA antiendomysial and gliadin antibodies were predictive of positive villous atrophy in 99.1% of patients • If both negative, normal mucosa in 99.1% of patients
Small Intestine Biopsy • Required for diagnosis before start of gluten-free diet • Panendoscopy/OGD with biopsies from 2nd or 3rd portion of the duodenum • Absent villi, hyperplastic crypts, increased numbers of intraepithelial lymphocytes • Reserve 2nd biopsy to unresponsive patients
Treatment • Strict Gluten-free diet for life • Avoid all foods with wheat, rye, barley • Avoid oats initially until remission • Avoid lactose initially until remission • Try foods containing wheat starch with gluten removed • Read all labels of foods, medications, etc • Avoid beer, ales, lagers, stouts • Wine, liquors, whiskey, brandy, spirits okay
Treatment • 70% improve within first two weeks • Full resolution of histology more common in children; 2-3 months after start of diet • Vitamin supplementation initially • May require IV corticosteroids if critically ill with celiac crisis especially if after a gluten challenge
References • Farrell and Kelly. “Celiac Sprue” NEJM. Vol 346 #3 January 17, 2002 • Hin et al. “Celiac Disease in Primary Care.” BMJ Vol 318 January 16, 1999 • Pruessner. “Detecting Celiac Disease in Your Patients.” Am Fam Phys March 1/98 • Gillett et al. “High Prevalence of Celiac Disease in Pts with Type I DM Detected by Antibodies to Endomysium and Tissue Transglutaminase.” Can Jour Gastroenterology May 2001