Download
1 / 70
720 likes | 973 Views
Coronary Artery Disease and Hypertension Williams’ Basic Nutrition and Diet Therapy Chapter 19 and American Heart Association. Cardiovascular Disease (CVD). Cardiovascular disease is the leading cause of death in the United States ( 650,000 deaths annually) Too many Americans Are overweight

E N D
Coronary Artery Disease and HypertensionWilliams’ Basic Nutrition and Diet TherapyChapter 19 and American Heart Association
Cardiovascular Disease (CVD) • Cardiovascular disease is the leading cause of death in the United States (650,000 deaths annually) • Too many Americans • Are overweight • Are sedentary • Smoke cigarettes • Manage stress ineffectively • Have uncontrolled high blood pressure • Have high cholesterol • Have diabetes or prediabetes • Do not know the signs of CVD
Major Forms of Cardiovascular Disease • Hypertension • Atherosclerosis • Coronary Artery Disease • Peripheral Vascular Disease • Congestive Heart Failure
Hypertension (HTN) • Too much force or pressure exerted against artery walls • Strains, weakens, and enlarges the heart • Scars and hardens arteries • Is very common (about 1 in 4 adults) • Often has no symptoms • Can usually be controlled with lifestyle and medication • Increases risk of heart attacks, strokes, kidney failure, and other health problems • Usually has no warning signs, so regular screening is critical
Atherosclerosis • Atherosclerosis begins in childhood and progresses at different rates, depending primarily on heredity and lifestyle choices such as smoking history, diet practices, physical activity, and stress. • The inner layers of artery walls are made thick and irregular by deposits of a fatty substance (plaque); the internal channels of arteries become narrowed and blood supply is reduced • Blockage of a coronary artery = heart attack • Blockage of a cerebral artery = stroke
Coronary Artery Disease (CAD) • Coronary Artery Disease (CAD) - Progressive plaque build up in the coronary arteries, disrupting blood supply to the heart - Total occlusion can lead to heart attack or sudden cardiac death • Arteriosclerosis:A form of atherosclerosis – hardening of the small arteries (arterioles) • Ischemia: Deficiency in blood to heart caused by Coronary Artery Disease
Peripheral Vascular Disease (PVD) • Damage or blockage in the peripheral arteries and veins which carry blood to the upper and lower extremities and organs in and below the stomach • PVD may cause: • Blood clots, inflammation, and narrowing or occlusion of blood vessels • Signs and symptoms: • Pain in the calves, thighs, and gluteal region • Angina • Intermittent Claudication- leg pain develops during walking and worsens with activity • Toes may turn blue; feet may be cold; pulse in leg is weak
Congestive Heart Failure (CHF) • Condition resulting from the heart’s inability to pump out all the blood that returns to it. Blood backs up in the veins leading to the heart, causing an accumulation of fluid in various parts of the body • Pulmonary Edema- “wet lungs” or accumulation of fluid in lung tissues • Caused by: • High blood pressure • Heart attack • Atherosclerosis • Birth defects • Rheumatic fever
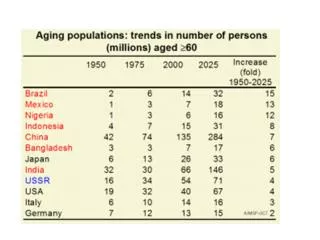
Cardiovascular Related Death in the U.S. Chapter 11
Non-Modifiable Risk Factors for Cardiovascular Disease • Family history (heredity) • Aging • Ethnicity • Latin Americans, Native Americans, Asian Americans, and African Americans • Gender: • Occurs more in men than women; after menopause women catch up with men in cholesterol level and potential heart disease risk
Gender and Cardiovascular Disease • Nearly 1 in 2 women die from CVD • Estrogen improves blood lipid concentrations and other risk factors in premenopausal women • Hormone replacement therapy is no longer recommended for CVD prevention in menopausal women • Women are more likely than men to die following a heart attack • Women are more likely than men to experience a heart attack without chest pain
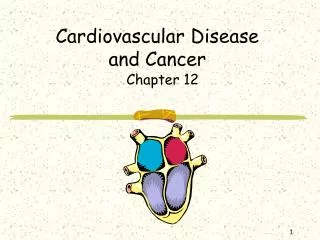
Annual Incidence of Heart Attack: Age and Gender Differences Chapter 11
Modifiable Risk Factors for Cardiovascular Disease • Hypertension • Elevated Cholesterol • Elevated Triglycerides • Vascular Inflammation • Smoking • Physical Inactivity • Obesity • Diabetes • Metabolic Syndrome • Psychological and Social Factors
Hypertension Guidelines Category Systolic Diastolic (mm Hg) (mm Hg) Normal below 120 and below 80 Pre hypertension 120–130 or 80–89 Hypertension Stage 1 140–159 or 90–99 Stage 2 160 and above or 100 and above
Hypertension • Pre-Hypertension: • No antihypertensive drug indicated • Lifestyle modification encouraged • Stage I • Antihypertensive drug (s) indicated • Stage II • Antihypertensive drug (s) indicated • Two drug combination for most
Treatment of High Blood Pressure • Increase physical activity • An individual can expect exercise-induced reductions of approximately 3 to 5 mm Hg in resting systolic and diastolic blood pressures (both through aerobic exercise and strength training) • Hypertensive people who are physically active have a lower risk of mortality from all causes than inactive individuals with normal blood pressure • The death rates for unfit individuals with low systolic blood pressure are much higher than for highly fit people with high systolic blood pressure
Treatment of High Blood Pressure • Weight control • A low-salt/low-fat and high potassium/high-calcium diet • Recommended salt intake: adequate = 1500 mg/day; limit = 2300 mg/day • Limit alcohol and caffeine intake • Smoking cessation • Stress management • Medication
The “D.A.S.H” Diet • Developed from the Dietary Approaches to Stop Hypertension landmark study (pg. 377) • 14 day diet to lower blood pressure. Average systolic decrease of 6 to 11 mmHg • Dailey Dietary Recommendations -Fruits= 4-6 servings -Vegetables= 4-6 servings -Dairy (low fat)= 2-3 servings -Lean Meats -High-Fiber Grains
Exercise Guidelines for Clients with Hypertension • Clients with Stage 1 or greater readings (140/90) should not be trained until their blood pressure is controlled and a physician has cleared them for exercise • Clients with controlled hypertension may participate in circuit weight training and aerobic exercise (walking, swimming…) • Clients may use free weights, weight machines, body weight, and elastic bands • No Isometric Exercises!
Exercise Guidelines for Clients with Hypertension • Goals: • Increase VO2 max • Increase ventilatory threshold:The air inspired into the respiratory tract and expired out of the respiratory tract • Increase caloric expenditure • Control blood pressure • Increase muscular endurance
Aerobic Exercise Guidelines for Clients with Hypertension • Intensity: 40-50% VO2 Max (according to research, low intensity exercise appears to be a more effective stimulus than moderate-intensity exercise training in reducing resting blood pressure responses to stress) ultimately attaining 50-85% VO2 Max • RPE should be 8-10 (6-20 scale) with a goal range of 11-13 • Duration: 15-30 minutes with a goal of 30-60 minutes • Frequency: 3-7 days per week • Weekly caloric expenditure will be between 700-2,000 calories
Resistance Training Guidelines for Clients with Hypertension • Frequency: 2-3 times per week on nonconsecutive days • Duration: 30-60 minutes per session • Intensity: • Low to moderate intensity • 16-20 reps • 1-3 sets • Rest intervals should be 2-3 minutes or longer to allow the client to fully recover between sets • Large-muscle, multijoint movements • Over time (6 months) the number of reps can decrease to 8-12 reps • Isometric Exercises are Contraindicated due to an increase in blood pressure
Elevated Cholesterol • Cholesterol is essential for the body and is an important component of cell membranes, sex hormones, vitamin D, protective nerve sheaths, and other body components • The body obtains cholesterol from food plus the liver manufactures it • Cholesterol is carried in the blood—to and from the liver—in lipoproteins
What Are Lipoproteins? • LDL=Low-Density Lipoproteins blood fats that transport cholesterol to organs and tissues; excess amounts result in the accumulation of deposits on artery walls • HDL=High-Density Lipoproteins blood fats that help transport cholesterol out of the arteries, thereby protecting against heart disease
Cholesterol Guidelines LDL cholesterol (mg/dl) Less than 100 Optimal 100–129 Near optimal/above optimal 130–159 Borderline high 160–189 High 190 or more Very high Total cholesterol (mg/dl) Less than 200 Desirable 200–239 Borderline high 240 or more High HDL cholesterol (mg/dl) Less than 40 Low 60 or more High (desirable)
Improving Cholesterol Levels • Habitual aerobic exercise: • > 6 METs, 3 times/week for 20 min/session • Lose body fat (if necessary) • Choose a diet low in fat, saturated fat, and cholesterol • Limit dietary cholesterol to less than 300 mg/day • Consume 25 to 38 grams of fiber per day, including a minimum of 10 grams of soluble fiber • Avoid foods that contain trans fatty acids, hydrogenated fat, or partially hydrogenated vegetable oil
Improving Cholesterol Levels • Limit egg consumption to less than 3 eggs per week • Bake, broil, grill, poach, or steam food instead of frying • Refrigerate cooked meat before adding to other dishes; remove fat hardened in the refrigerator before mixing meat with other foods • Avoid fatty sauces made with butter, cream, or cheese • Consider drug therapy if the above fail to decrease LDL cholesterol
Cholesterol Medications • Statins (HMG CoA reductase inhibitors) • Block HMG Coenzyme-A in liver to reduce production of cholesterol in individuals who are unable to adequately control through diet and exercise *Statins are the most widely prescribed medications in the U.S. Ex: Crestor (rosuvastatin), Lipitor (atorvastatin), Zocor (simvastatin)
Cholesterol Medications • Cholesterol Absorption Inhibitor- Block the reabsorption of LDL cholesterol in liver (reverse transport). Ex: Zetia • Lipid Regulating Agents- Improve Omega 3-acid ethyl esters, increase HDL and improve “clean up” of LDL cholesterol in bloodstream. Ex: Lovaza • Bile Acid Sequestrants- Block LDL cholesterol reabsorption in bile acid from liver. Ex: Questran • Nicotinic Acid Derivatives- Increase free floating niacin to improve HDL cholesterol. Ex: Niaspan
Elevated Triglycerides • Manufactured mainly in the liver, from refined sugars, starches, and alcohol • Found in poultry skin, lunch meats, and shellfish • Contributing factors include many of the same factors that increase cholesterol levels; excess alcohol intake and very high carbohydrate diets also raise triglyceride levels Triglycerides (mg/dl) Less than 150 Normal 150–199 Borderline high 200–499 High 500 or above Very high
Triglyceride Medications • Fibrates • Lower triglycerides in individuals who are unable to adequately control through diet and exercise. Usually used in conjunction with a cholesterol lowering agent. Ex: Tricor, Antara
Vascular Inflammation • Clinical data shows that inflammation is a major risk factor for heart attacks • Low-grade inflammation can occur in a variety of places throughout the body • For years it has been known that : • Inflammation plays a role in CHD • Inflammation hidden deep in the body is a common trigger of heart attacks, even when cholesterol levels are normal or low and arterial plaque is minimal
Vascular Inflammation • C-Reactive Protein (CRP) is a protein whose blood levels increase with inflammation • Physicians have turned to CRP to evaluate ongoing inflammation in the body • People with elevated CRP are more prone to cardiovascular events • The risk of a heart attack is even higher in people with both elevated CRP and cholesterol, resulting in an almost 9-fold increase in risk
Vascular Inflammation • CRP levels decrease with statin drugs • Also helpful are exercise, weight loss, proper nutrition, and aspirin • Omega-3 fatty acids inhibit proteins that cause inflammation • Excessive intake of alcohol and high protein diets increase CRP • Aspirin therapy may also help control inflammation
Smoking • Smoking • Reduces levels of HDL (“good” cholesterol) • Raises levels of LDL (“bad” cholesterol) and triglycerides • Nicotine raises blood pressure causing blood flow to impede • Displaces oxygen in the blood • Exposure to environmental tobacco smoke (ETS) also increases CVD risk, causing more than 50,000 deaths per year among nonsmokers
Smoking • Smoking speeds up the process of atherosclerosis • Causes a threefold increase in the risk of sudden death following a myocardial infarction • As far as the extra load on the heart is concerned, giving up one pack of cigarettes per day is the equivalent of losing between 50 and 75 pounds of excess body fat!
Physical Inactivity • Epidemiological evidence shows that physical inactivity doubles the risk of CAD • Aerobic training adaptations: • Produces larger coronary arteries • Increases heart size • Increases heart pumping capacity • Improves circulation of blood to vessels surrounding heart • Reduces blood pressure in individuals with moderate hypertension • Improves blood lipids and their ratios • Reduces insulin resistance
Obesity • A BMI of 30 or higher recognized as a major risk factor for coronary heart disease • Excess body fat contributes to • High blood pressure • Elevated cholesterol levels • Diabetes • Narrowing of coronary arteries • Fat that collects in the torso (“apple” shape) is more dangerous than fat that collects around the hips (“pear” shape)
Diabetes • Disruption of glucose metabolism, resulting in increased blood levels of glucose; pre-diabetes also increases CVD risk • Damages the lining of arteries • Diabetes is linked to other CVD risk factors • Diabetes increases CVD risk even if glucose and insulin levels are under control
Metabolic Syndrome • Hypertension, coronary artery disease, abnormal blood lipids, type 2 diabetes, and upper body obesity are linked through the common pathway of insulin resistance and hyperinsulinemia. • Metabolic syndrome, syndrome X, and civilization syndrome are terms used to describe this interrelationship
Metabolic Syndrome • As cells resist insulin’s action, the pancreas releases even more insulin in an attempt to keep blood glucose from rising • A chronic rise in insulin appears to trigger a series of abnormalities referred to as metabolic syndrome or syndrome X • These abnormal conditions include • Low HDL cholesterol, high triglycerides, an increased blood clotting mechanism, and high blood pressure
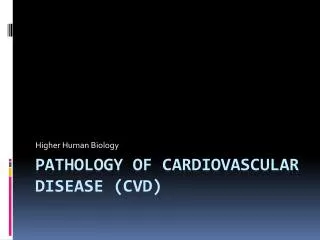
Metabolic Syndrome is identified by the presence of at least three of the components Chapter 11
Psychological and Social Factors • Stress • Chronic hostility and anger • Suppressing psychological distress • Depression and anxiety • Social isolation • Low socioeconomic status
CARDIOVASCULAR TERMINOLOGY • Angina Pectoris: chest pain, vague arm neck, back pain • Stroke: Blockage of blood vessels supplying the brain • Myocardial Infarction (MI): Heart attack due to ischemia (blockage, narrowing, plaque rupture) • Hypoxia: Reduced oxygen supply
Cardiovascular Terminology • Dyspnea: Difficulty breathing, may indicate left ventricular failure • DOE=Dyspnea on exertion • SOB=Short of breath • Hypotension: Low blood pressure • Systolic pressure (top number) is less than 90 • Results in dizziness • Atrial Fibrillation (A-Fib): Asynchronous contraction of the atrial muscle fibers so atrial pumping ceases altogether
Stroke • An impeded blood supply to some part of the brain results in the destruction of brain cells; a cerebrovascular accident (CVA) • Ischemic stroke = caused by blood clot • Hemorrhagic stroke = caused by ruptured blood vessel • Can be fatal or cause permanent disability
Warning Signs of a Stroke • Sudden numbness or weakness in the face, arm and/or leg, especially on one side of the body • Sudden confusion, trouble speaking or understanding speech • Sudden trouble seeing, including double vision, blurred vision or partial blindness, in one or both eyes • Trouble walking, dizziness, loss of balance or coordination • Sudden severe, headache with no known cause.