Proteinuria
Proteinuria. The primary care approach Presented by feras ghosheh 6 th Y medical student AL-QUDS UNIVERSITY. 4MedStudents.com. Proteinuria. INTRODUCTION DEFINITION EPIDEMIOLOGY PATHOGENESIS DIFFERENTIAL DIAGNOSIS CLINICAL FEATURES Specific Entities INVESTIGATIONS MANAGEMENT.

Proteinuria
E N D
Presentation Transcript
Proteinuria The primary care approach Presented by feras ghosheh 6th Y medical student AL-QUDS UNIVERSITY 4MedStudents.com
Proteinuria • INTRODUCTION • DEFINITION • EPIDEMIOLOGY • PATHOGENESIS • DIFFERENTIAL DIAGNOSIS • CLINICAL FEATURES • Specific Entities • INVESTIGATIONS • MANAGEMENT 4MedStudents.com
INTRODUCTION The protein is found in normal urine, and it’s divided into: 1-60% plasma proteins: albumin (major) IgG, IgA ,light chains ,heavy chains , transferrin ,haptoglobin ,lysozyme ,amylaze ,kallikrein. 2- 40% originating from the secretions of the urinary tract including: tamm-horstall ,urokinase and secertory IgA. The reasonable upper limit of normal protien excretion in healthy children = 150 mg/24 hrs.
DEFINITION • The excretion of an excessive amount of protein (>150mg/day) in the urine as defined by qualitative, semi-quantitative, and quantitative methods.
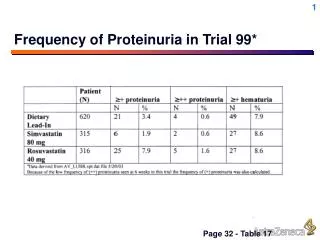
EPIDEMIOLOGY • incidence: 1 - 5% (depend upon age and number of samples) • prevalence: 5 - 11% (1+ proteinuria) • only 10% of kids with proteinuria will have abnormalities after 6-10 month of follow-up • of those children with isolated proteinuria, <2% will have significant underlying renal disease • the incidence of proteinuria in patients with underlying renal disease is remarkably high
PATHOGENESIS There are three basic types of proteinuria : 1-glomerular 2-tubular 3- overflow
1. Glomerular • mechanisms: • . increased GFR • . increased glomerular permeability • basement membrane • endothelial, epithelial cell injury • electrostatic charge barrier • proteins: larger macromolecules, albumin
2. Tubulointerstitial • impaired tubular reabsorption of filtered proteins • proteins: low MW proteins, lysozyme, B2-microglobulin • Tamm-Horstall protein
3. Overload Proteinuria • increased load overloads tubular reabsorptive capacity • proteins: low MW plasma proteins, Ig light chains, myoglobulin, lysozyme, albumin
1. Benign Proteinuria a. Benign Transient Proteinuria b. Orthostatic Proteinuria c. Persistent Asymptomatic Proteinuria
2. Pathologic Proteinuria A- Glomerular 1. Hereditary 2. Non-Hereditary B-Tubulointerstitial 1. Hereditary 2. Non-Hereditary
1. Hereditary Congenital Nephrotic Syndrome Alport Syndrome 2. Non-hereditary Acute (GN) -Poststrep GN -H.U.Syndrome -H.S. Purpura 2. Chronic 1. Primary Minimal Change Disease* FSGN Mesangioproliferative GN Membranous GN Membranoproliferative GN 2. Secondary Berger (IgA) Nephropathy Goodpastures Nephropathy SLE Nephropathy Wegeners Nephropathy Diabetic Nephropathy Renal Vein Thrombosis Sickle Cell Disease A- Glomerular
1.Hereditary Cystinosis Galactosemia Lowe Syndrome Medullary Cystic Kidney Proximal RTA Wilson Disease 2. Non-Hereditary Acute Tubular Necrosis analgesic abuse antibiotics cystic diseases heavy metal poisoning homograft rejection hypokalemia interstitial nephritis penicillamine reflux B-Tubulointerstitial
3. Overload Proteinuria 1. Neoplastic Amyloidosis Leukemia (monocytic, monomyelocytic) - lysozymuria Multiple Myeloma Waldenstrom's Macroglobinemia 2. Others IDDM (microalbuminuria) repeated albumin or blood transfusions Rhabdomyolysis most common causes of proteinuria in childhood
CLINICAL FEATURES: 1. History of Presenting Illness • at the end of the history, one should be able to discern: 1. benign vs pathologic proteinuria (if pathologic then) 2. glomerular vs tubulointerstitial proteinuria (if glomerular then) 3. hereditary vs non-hereditary (if non-hereditary then) 4. acute GN vs chronic GN (if chronic then) 5. primary GN vs secondary GN 6. nephrotic vs non-nephrotic proteinuria 7. proteinuria with or without hematuriauria • onset when began with conditions identified around the initial presentation, i.e., drug ingestion record of previous urinalyses • precipitation/palliation identification of triggering agents infectious, drugs, foods, chemicals, vaccinations helps to identify acquired forms of tubulointerstitial proteinuria
quality associated with hematuria severity more likely to be pathologic proteinuria if associated with hematuria or Nephrotic Syndrome (edema, hypoalbuminemia, hypercholesterolemia) if Nephrotic Syndrome present: likely to be a primary GN unlikely to be benign etiology or secondary GN timing acute vs acute-on-chronic intermittent vs persistent duration of proteinuria associated symptoms past medical history functional inquiry helps to differentiate acute GN from chronic GN helps to identify overload proteinuria causes
Family History helps to differentiate hereditary from non-hereditary forms of both glomerular and tubulointerstitial forms of proteinuria: 1. Proteinuria family members must have had previous urinalysis to ascertain this 2. Renal Disease Polycystic Kidney Disease Nephrotic Syndrome, Fanconi Disease renal dialysis kidney transplantation 3. Others hearing/ocular impairment (Alport Syndrome)
Specific Entities 1. Benign Transient Proteinuria • benign proteinuria associated with precipitating factors - fever, exercise, stress, cold weather, dehydration, high blood pressure, seizures, etc Orthostatic Proteinuria2. • diagnosis based upon the Postural Test • has a benign clinical course
3. Persistent Asymptomatic Proteinuria proteinuria that persists for 3-6 months renal biopsy after 6 months of persistent proteinuria and if FSGS then at risk for chronic renal failure 4. Congenital Nephrotic Syndrome onset at birth with Nephrotic Syndrome (massive proteinuria, hypoalbuminemia, edema, and hyperlipidemia) very difficult to treat with poor prognosis 5. Poststreptococcal GN proteinuria + hematuria associated symptoms prodrome of pharyngitis, URTI, impetigo Nephrotic and/or Nephritic Syndrome
6. Hemolytic Uremic Syndrome proteinuria + hematuria associated symptoms prodrome of bloody diarrhea anemia and thrombocytopenia (petechiae) Nephrotic and/or Nephritic Syndrome 7. Henoch-Schoenlein Purpura proteinuria + hematuria associated symptoms purpuric rash, arthritis, abdominal pain Nephrotic and/or Nephritic Syndrome 8. Primary Glomerulonephritis isolated proteinuria +/- Nephrotic Syndrome associated symptoms edema, hypoalbuminemia, hyperlipidemia
9. Secondary Glomerulonephritis proteinuria +/- hematuria associated with a disease entity, i.e., SLE, Goodpastures Disease, Wegeners Disease, Diabetes Mellitus 10. Hereditary Tubulointerstitial Proteinurias tubular proteinuria associated symptoms episodes of vomiting, dehydration, weakness, fever, anorexia, constipation, failure to thrive, polydipsia, polyuria
INVESTIGATIONS 1. Proteinuria (Diagnosis) 1. Qualitative - Dipstick • measures a range of protein concentrations • depth of colour increases in a semiquantitative manner with increasing urinary protein concentration • to rule out false positives must have: • 3 samples with proteinuria • first voided early morning samples • pH < 6.0 with known specific gravity • 1+ (72-240 mg/24 hrs) or greater is considered abnormal • dependent on specific gravity of urine sample • FP: gross hematuria, highly alkaline urine, UTI
2. Semi-quantitative - Protein/Creatinine Ratio in Urine • random early morning single voided specimen • children < 2 years : < 0.5 • children > 2 years : < 0.2 • nephrotic : > 3.5 • correlates with the 24 hour protein excretion data
3. Quantitative - 24 hr. urine collection gold standard if dipstick is 1+ or more than obliged to do a 24 hour urine collection 24 hr. urine collection Protein (mg)/m2/hr < 4 mg/m2/hourr (normal) 4-40mg/m2/hour (proteinuria) 40 mg/m2/hour (nephrotic) Protein (mg)/24 hr 2 to 12 months : > 155 mg/24 hr 3 to 4 years : > 140 mg/24 hr 4 to 10 years : > 190 mg/24 hr 10 to 16 years : > 250 mg/24 hr FP: radiographic contrast media, cephalosporins, pencillin analogues, sulfonamide metabolites
2. Indications for Further Investigation • Non-orthostatic Proteinuria • Persistent Proteinuria • Symptomatic (edema, elevated BP, abdominal pain, hematuria)
3. First Line Investigations 1. Urinalysis R&M, C&S, microscopy orthostatic test 24 hour collection total protein creatinine clearance 2. Serum electrolytes, BUN, creatinine, albumin, cholesterol, triglyceride, calcium, protein, CBC orthostatic test 4. Second Line Investigations 1. Urine protein electrophoresis can be used to differentiate glomerular (albumin) from tubular (Tamm-Horstall) proteinuria 2. Serum IgA, PTH, ANA, protein electrophoresis, ASOT, anti-GBM antibodies, uric acid, C3, C4 3. Imaging Studies renal ultrasound to rule out renal vein thrombosis 4. Renal Biopsy indicated for: progressive proteinuria with hematuria all forms of Nephrotic Syndrome except that caused by steroid-responsive Minimal Change Disease
MANAGEMENT • treat underlying disorder • treat complications
Thank you 4MedStudents.com