Streptococcus pneumoniae and Staphylococci
260 likes | 819 Views
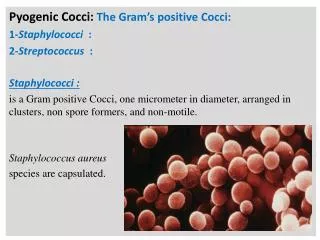
Streptococcus pneumoniae and Staphylococci. Faculty: Dr. Alvin Fox. Suggested reading: Murray, Third edition Chapters 22 and 23. S. pneumoniae Diplococcus Pneumococcus Autolysin Bile solubility test Optochin susceptibility Capsule Quellung reaction. Staphylococcus aureus

Streptococcus pneumoniae and Staphylococci
E N D
Presentation Transcript
Streptococcus pneumoniaeand Staphylococci Faculty: Dr. Alvin Fox Suggested reading: Murray, Third edition Chapters 22 and 23
S. pneumoniae Diplococcus Pneumococcus Autolysin Bile solubility test Optochin susceptibility Capsule Quellung reaction Staphylococcus aureus Staphylococcus epidermidis Coagulase (+) or Coagulase (–) ,,and and cytotoxins Leucocidin Lipase Exfoliatin Enterotoxins Toxic shock syndrome Toxic shock toxin Protein A KEYWORDS
S. pneumoniae Streptococcus pneumoniae in spinal fluid. FA stain (digitally colorized).CDC/Dr. M.S. Mitchell
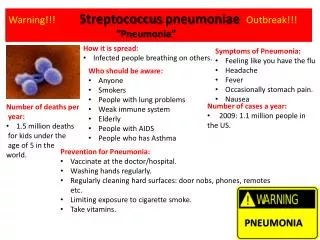
S. pneumoniae is a leading cause of pneumonia in • all ages (particularly the young and old), often • after "damage" to the upper respiratory tract • (e.g. following viral infection). • It also causes middle ear infections (otitis media). • The organism often spreads causing bacteremia and meningitis.
S. pneumoniae is hemolytic and there is no group antigen. • Direct Gram staining or detection of capsular antigen in sputum can be diagnostic. • The organism grows well on sheep blood agar.
Autolysin • Pneumococci are identified by solubility in bile. • An autolysin (peptidoglycan degrading enzyme) is released by bile from the cell membrane and binds to a choline-containing teichoic acid attached to the peptidoglycan. • The autolysin then digests the bacterial cell wall resulting in lysis of the cell.
If the cells are grown in ethanolamine instead of choline, ethanolamine is incorporated into the teichoic acid. • The autolysin then cannot lyse the cell wall. • Understanding how the autolysin works has led to the suggestion that antibiotics (including penicillin) work together with the autolysin in killing of pneumococci in vivo. • The organisms are also identified by susceptibility to optochin (ethyl hydrocupreine).
The optochin test is a presumptive test that is used to identify strains of Streptococcus pneumoniae. Optochin (ethyl hydrocupreine) disks are placed on inoculated blood agar plates. Because S. pneumoniae is not optochin resistant, a zone of inhibition will develop around the disk where the bacteria have been lysed. This zone is typically 14mm from the disk or greater. Not optochin sensitive optochin sensitive
Capsule • This is highly prominent in virulent strains and its carbohydrate antigens vary greatly in structure among strains. • The capsule is anti-phagocytic and immunization is primarily against the capsule. • Capsular vaccines are available for susceptible individuals; immunity is serotype-specific.
Using appropriate type-specific antisera, the capsule on isolated bacteria can be "fixed" and becomes visible microscopically (the Quellung reaction) Quellung reaction: Swelling of the capsule surrounding a bacterium as a result of interaction with anticapsular antibody, consequently the capsule becomes more refractile and conspicuous. • The Quellung reaction is useful in microbial identification.
The organism also produces pneumolysin that degrades red blood cells under anaerobic conditions (observed as hemolysis). • Complement activation by teichoic acid may explain the attraction of large numbers of inflammatory cells to the focal site of infection. • Most strains of S. pneumoniae are susceptible to penicillin. However, resistance is quite common.
Gram positive • Facultative anaerobes • Occur in grape like-clusters • Catalase positive • Major components of the normal flora of skin and nose.
One of the commonest causes of opportunistic • infections in the hospital and community; • including pneumonia • osteomyelitis • septic arthritis • bacteremia • endocarditis • abscesses/boils • other skin infections
(ii) Food poisoning. • The food becomes contaminated with the • organism from human contact, grows and • produces enterotoxin. • The organism does not "infect" on ingestion • of food. • Onset and recovery both occur within a few • hours. • Vomiting, nausea, diarrhea and abdominal pain are present.
(iii) Healthy people: • boils (iv) Exfoliative toxin causes scalded skin syndrome in babies.
Box of Rely tampons.Associated with outbreak of toxic shock syndrome. CDC
(v) Toxic shock syndrome particularly after tampon use includes: • fever • rash • desquamation • vomiting • diarrhea • Toxic shock toxin is involved. • The organism does not disseminate. • However, the toxin does and is responsible for the clinical features.
Identification 1. hemolytic on sheep blood agar 2. Mannitol fermentation 3. Golden pigmented (aureus)- often 4. Coagulase-positive 5. In reference laboratories phage-typing is used.
S. aureus causes a number of different disease • entities associated with production of certain • exotoxins. • In addition to these "disease-specific" exotoxins, • other cell lytic exotoxins include: 1. toxin 2. [sphingomyelinase C] 3. toxin 4. toxins and leucocidins
Some tissue-degrading enzymes may be involved in spreading (e.g. lipase and hyaluronidase). • Free protein A binds to immunoglobulin and • complement, blocking Fc and complement • receptors and is thus anti-phagocytic.
Staphylococcus epidermidis • Staphylococcus epidermidis is a less common • cause of opportunistic infections than S. aureus, • but is still significant. • It is a mediator of nosocomial infections: • catheters • shunts • surgery {e.g. heart valves} • It is a major component of the skin flora and thus • commonly a contaminant of cultures.
Identification 1. Non-hemolytic on growth on sheep blood agar 2. Does not ferment mannitol 3. Non-pigmented 4. Coagulase-negative
Staphylococcus saprophyticus • A significant cause of urinary tract infections. • Coagulase-negative and not usually differentiated • from S. epidermidis clinically
Antibiotic therapy • Staphylococci (including both coagulase positive and coagulase negative organisms) can produce a phage-coded penicillinase that degrades beta lactam antibiotics. • Some strains also have modified penicillin binding • proteins. • lactam antibiotics (including methicillin) are • often ineffective. • Vancomycin is the drug of choice.