Download
1 / 35
410 likes | 606 Views
This article explores the two main types of adrenergic receptors—alpha and beta—and their roles when activated by adrenergic agonists. Alpha receptors typically induce excitatory responses, while beta receptors mainly result in inhibitory effects. We delve into the pharmacological actions and classifications of adrenergic agonists, including catecholamines and non-catecholamines. The discussion covers how these drugs affect cardiovascular function, gastrointestinal smooth muscle, the respiratory system, and the genitourinary tract, highlighting their therapeutic implications and potential side effects.

E N D
Adrenergic Agonist By: Dr.ALTWIJRY
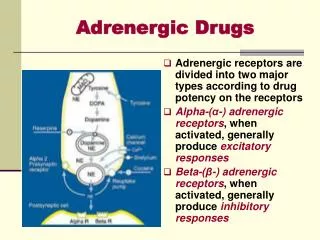
Adrenergic receptors are divided into two major types according to drug potency on the receptors Alpha-(α-) adrenergic receptors, when activated, generally produce excitatory responses Beta-(β-) adrenergic receptors, when activated, generally produce inhibitory responses Adrenergic Drugs
α α 1 2 Type “Vascular” “Presynaptic” Distribution Blood vessels, GIT , sphincters, Autonomic nerve terminals, blood iris radial, liver vessels, pancreatic islets, platelets Receptor - G PCR , linked to activation of G PCR , linked to inhibitio n of q i Transduction PLC - DAG - IP adenyl cyclase - c.AMP 3 Agonist E≥NE>>>I SOP E≥NE>>> ISOP Profile α - MeDOPA Selective Phenylephrine & methoxamine Clonidine, Agonists Selective Prazocin Yohimbine Antagonists -Adrenergic Receptors
Direct-acting Adrenergic AgonistsA. Catecholamines • Catecholamines, adrenergic neurotransmitters; L-norepinephrine (NE), L-epinephrine (E), & L-dopamine (DA) in addition to the synthetic analog isoproterenol • They have the following characteristics: • High potency • Rapid enzymatic inactivation by MAO & COMT as well as neuronal & non-neuronal uptake • Therefore they have short duration when given parenterally and are inactive orally • Poor ability to pass the CNS (Polar) • COMT & MAO can be in gut wall, also MAO can be in the live
Direct-acting Adrenergic AgonistsB. Non-catecholamines • Non-catecholaminesare adrenergic agonists lacking the catechol hydroxyl groups • Therefore they are of longer duration, can be given orally and they are not inactivated by COMT, poor substrate for MAO • They include agents like phenylephrine, ephedrine and amphetamine
General Mode of Action of Adrenergic Agonists • Direct-acting agonists that act directly by binding to the adrenergic receptors, include NE, E, DA, phenylephrine & isoproterenol • Indirect-acting agonists that cause the release of NE from intra-neuronal storage vesicles by the virtue of being taken up by the pre-synaptic adrenergic neurons • They include agents like amphetamine and tyramine • Mixed-action agonists, ephedrine
Pharmacological ActionsA. Nonselective Direct-acting Adrenergic Agonists 1- Cardiac Effects • Increased force of contraction(positive inotropic effect) • Enhanced automaticity of latent pacemaker cells that may lead to arrhythmias • Acceleration of impulse conduction velocity(conductivity) between the atria and ventricles via shortening of the refractory period of the A-V node • Increased stroke volume and cardiac output but with accompanied rise in oxygen consumption • The heart efficiency (performance) is decreased in terms of lower cardiac work in relation to oxygen consumed • Reflex bradycardia, NE, and E but in high doses (blocked by ATROPINE)
In vivo (Iv) Reflex bradychardia . • In vivo + atropine Tachycardia . • here the vagus nerve is blocked be atropine . • In vitro (heart outside the body) Tachycardia . • Β1 is more predominant in the heart .
2) Vascular Smooth Muscle Effects • NE constricts all blood vessels except the coronary vascular bed (α>β2) • E has mixed effects according to the vascular bed (β2> α), dilation in skeletal muscles, liver & coronaries • Isoprenaline has purely vasodilatotory effects (β2>>> α) • E constrict arterioles in the skin, mucus membrane, and viscera (α affect). • E dilates arterioles in the liver and skeletal muscle (β2 affect). • Vascular in skeletal muscle has α1 and β2, while β2 is predominantbut in high dose of E vasoconstriction .
Effects of I.V. infusion of Epinephrine, Norepinephrine & Isoprenaline in Humans
3- Effects on Gastrointestinal Tract Relaxation of GIT smooth muscle through • Inhibition of the release of ACh from cholinergic neurons via activation of α2-adrenoceptors on cholinergic nerve terminals • Stimulation of β2-receptors, activates adenyl cyclase-c.AMP- PKA cascade leading phophorylating inactivation of myosin-light chain kinase enzyme • Stimulation of α1-adrenoceptors causes increased potassium channel activity resulting in increased K+ conductance & hyperpolarization
4- Effects on Respiratory System • β2-Adrenoceptors stimulation leads to relaxation (inhibition) of bronchiolar smooth muscle and bronchodilation, and hence lowering airway resistance (Asthma) • Inhibition of antigen-mediated production of inflammatory mediators of asthma via β2-adrenoceptorsstimulation (Asthma) • α1-Adrenoceptors activation results in vasoconstriction of the upper respiratory tract mucous membranes and hence lowering congestion (Nasal decogestant) • NE is never used for bronchospasm .
5- Effects on the genitourinary system • Uterus • They are dependent on the uterine status • Norepinephrine increases the rate of contraction of pregnant human uterus • Epinephrine inhibits uterine tone and contractions during the last month of pregnancy as well as at parturition • This observation is the basis for the use of β2-adrenoceptors agonists to delay premature labor
5- Effects on the genitourinary system • Urinary Bladder • 1-adrenoceptors show • High density in smooth muscle of urethera & prostate • Selective 1-adrenoceptor antagonists are used for treatment of urinary retention in benign prostatic hypertrophy
6- Effects on the Eye • Stimulation of α1-adrenoceptors on the radial smooth muscle of the iris leads to pupil dilation (mydriasis), theoretically result in blocking of drainage of aqueous humor and increase of IOP • α1-adrenoceptors stimulation results in vasoconstriction that in turn causes inhibition of the formation of aqueous humor & lowering of IOP (no cycloplegia) • -blockers (timolol) decrease the formation of aqueous humor & used topically in glaucoma treatment
7- Metabolic Effects • Lipolysis & thermogenesisare stimulated leading to increased breakage of triglcerides into free fatty acids and glycerol through activation of lipase enzymatic activity (β1/ β3-adrenergic receptor stimulation-increased c.AMP-PKA activation -phosphoryaltion of lipase) • Hepatic & Skeletal Muscle Glycogenolysisare stimulated resulting in hyperglycemia & increased plasma glucose & lactic acid (β2-adrenergic receptor stimulation with subsequent activation of adenyl cyclase-c.AMP-PKA cascade-Activated PKA phosphorylates phosphorylase kinase - activates phosphorylase) • Gluconeogenesis is stimulated as well • Calorigenic action where oxygen consumption is increased in response to catecholamines mainly via increased oxidisable substrate from increased lipolysis
Endocrine Glands • Insulin release is stimulated via 2-adrenoceptors & inhibited by -receptors • Insulin R activity is decreased by 1-receptors through decreased GLUT4 translocation • Glucagon secretion is increased by sympathetic stimulation • Renin release from juxtaglomerular appartatus is stimulated via 1-adrenoceptors • Epinephrine:increase lipolysis Hyperglycemia increase glycogenesis (β2-liver )increase glycogenolysis (β2-liver)decrease insuline releas (α2-pancrease)
Central Nervous System (CNS) • Catecholamines are powerful CNS stimulants • Cocaine & amphetamine euphoric effects are mediated via increase CA brain levels due to uptake blockade/enhanced release respectively • Side effects of adrenergic agonists may include anxiety, nervousness, & tremors while antagonist may enhance depression. • Ampetamine is a drug abuse only and it is not used by another person.
Skeletal Muscles • 1-agonists (E & dobutamine) facilitate Ach release from motor neurons possibly via c.AMP-PKA- N-channels activation, hence increase muscle activity (myasthenia gravis) • 2-agonists (E & salbutamol) cause propranolol-sensitive muscle tremors possibly via hypokalemia & increased muscle activity.(Hypokalemia & increased muscle activity are side affects) • When we use β2-agonist for bronchospasm patient the patient may have a mild tremor then his muscle will be sensitive to propanolol.
Selective α1-Adrenergic Agonists Phenylephrine & methoxamine, metaraminol, mephentermine • elevated systolic & diastolic BP • increased total peripheral resistance • barororeceptor mediated reflex decrease in heart rate via enhancement of vagal activity • They are less potent but longer acting than norepinephrine, being non susceptible to metabolism with COMT
Therapeutic Uses of α1-Adrenergic Agonists • Local nasal decongestantto produce vasoconstriction of nasal mucosal vasculature • Treatment of supraventricular tachycardia arising in AV node and atria • They elevate blood pressure & stimulate vagal activity via baroreceptor-mediated reflex action (α1-agonists have not direct affect on the heart) • To overcome hypotension induced by some general anesthetic agent
α2 -Adrenergic Agonists • Clonidine & α-methyldopa activate α2-Adrenergic receptorsin the lower brain stem (nucleus of tractus solitaries) leading to decreased central outflow of the sympathetic nervous system • Peripherally, they decrease NE release by stimulation of presynaptic α2-Adrenergic receptors • Oral intake produces a prolonged hypotensive response (Treatment of Hypertension) • IV injection raises BP by direct stimulation of postsynaptic α1- & α2-Adrenergicreceptors • In addition, α-methyldopa is taken up by adrenergic neurons and synthesized into α-methylnorepinephrine which is a false adrenergic transmitter
α2 -Adrenergic Agonists • They are used in management of hypertension • Clonidine does not induce postural hypotension • Clonidine can cause “rebound hypertension” upon sudden stop, prior treatment with phentolamine (-blocker) protects against • Small doses of clonidine are effective as prophylactic therapy of migraine • Dry mouth & constipation are most frequent side effects (inhibition of cholinergic neuronal activity) • Apraclonidine is used as adjuvant therapy for glaucoma via decrease of aqueous humor formatiom
β1-Adrenergic Agonists • Dobutamineis a synthetic dopamine analog. It is a selective β1-adrenergic agonist. On the heart, it produces a more pronounced positive inotropic effect than its chronotropic effect when compared to dopamine. There is no defined reason for such differential action • Therapeutic use of dobutamine is based on its ability to increase cardiac output via the positive inotropy with little effect on heart rate and myocardial oxygen consumption • Hence, it is used in cardiogenic shock and decompensated heart failure
Dopamine Dopamine is better than NE in shock treatment because it raises blood pressure and enhance perfusion of the kidney and splanchnic areas while NE decreases blood supply to the kidney which lead to renal shutdown Use with it diuretics because it causes Na-water retention It is dose dependent ( review the book page 75 Lippincott)
β2 adrenergic receptor agonists • Terbutaline, albuterol (salbutamol), pirbuterol & ritodrineare selectiveβ2 adrenergic receptor agonists with little effect on β1 cardiac receptors • Hence, they have the advantage of producing bronchodilation without cardiac stimulation • They produce uterine relaxation • They are given orally, IV or by inhalation & have no CNS stimulation • Salmeterol & formoterol are long-acting agonists • Fenoterol is an intermediate-acting (8 hrs)
β2-Adrenergic Receptor Agonists • Orciprenaline (metaprotrenol, Alupent R) is relatively a selective agonist used both by oral & inhalation • Therapeutic uses of β2 adrenergic receptor agonists • Treatment of bronchial asthma and bronchospasm associated with bronchitis and emphysema • Delay delivery in premature labor and in threatened abortion; ritodrine is frequently used for this purpose
Indirect- & Mixed-Acting Adrenergic Receptor Agonists • Ephedrine (it is rarely used in the clinic) • Chemically related to EP and stimulates release of NE • It is not a substrate forCOMT or MAO & hence has long duration of action • It activates β2 as well as α- and β1-aderenergic receptors • It is used to treat mild cases of asthma • It crosses BBB giving rise to CNS stimulant action • It is now replaced by more selective β2 agonists • Tyramine (it is not used) in cheese, fermented sausage & wines • It enters synaptic vesicle and causes displacement & release of NE & normally degraded by MAO • MAO inhibitors in conjunction with tyramine-containing foods may lead to rapid release of NE & severe hypertension
Indirect- & Mixed-Acting Adrenergic Receptor Agonists • Pseudoephedrine & Phenylpropanolamine • They stimulate the release of NE • They are used as over-the-counter (OTC) nasal decongestants for symptomatic relief of hay fever and rhinitis • Pseudoephedrine has little β2 agonist activity, limited CNS stimulation • Phenylpropanolamine also used to relieve upper respiratory conditions associated with common cold
Clinical uses of α- & β-Adrenergic Agonists • Nasal decongestant: Vasoconstriction in nasal mucous membranes by α1-agonists like phenylephrine, pseudoephedrine & xylometazoline • Treatment of hypotension • Selectiveα1-agonistslike phenylephrine, methoxamine & mephentermine are administered parenteraly to elevate blood pressure in hypotension accompanying spinal anesthesia. They cause prompt vasoconstriction increasing total peripheral resistance and hence raising diastolic and systolic pressures • In hypovolemic shock use of α1-agonistshas the potential to cause further impairment of microcirculation already affected by high level of catecholamine release So α1-agonists are not used in hypovolemic shock and we have to use fluids
Clinical uses of α- & β-Adrenergic Agonists • Cardiogenic shock (MI), NE, dobutamine or DA • NE is given by ONLY IV infusion at doses that raise BP, and increase cardiac contractility without serious vasoconstriction • Dopamine is advantageous in producing splanchnic and renal vasodilation (D receptors), increasing glomerular filtration and urine production • Dobutamine is more or less similar to dopamine being more selective on cardiac β1-adrenergic receptors
Clinical uses of α- & β-Adrenergic Agonists • Anaphylactic Shock: Epinephrine is of choice given by SC route to reverse the histamine-induced broncho-constriction & hypotension • Opthalmic Uses: • Mydriatics: phenylephrine & ephedrine may be used for eye examination • Glaucoma: phenylephrine or epinephrine may be used locally to decrease IOP
Clinical uses of α- & β-Adrenergic Agonists • 5- Respiratory uses: • Treatment of asthma using theselective β2 adrenergic receptor agonists including terbutaline, albuterol and orciprenaline by oral route or by inhalation. They have fewer cardiovascular stimulant effects • Relieve of congestion of upper respiratory tract in hey fever and rhinitis. For this purpose, α1 agonists such as phenylephrine, pseudoephedrine & phenylpropanolamine can be used orally to produce vasoconstriction of mucous membrane vasculature
Clinical uses of α- & β-Adrenergic Agonists • As Vasoconstrictors with Local Anesthetics: Epinephrine and phenylephrine may be used to produce localized vasoconstriction which inhibits systemic absorption and lower bleeding • Epistaxis; Epinephrine (1:100,000 dilution) or -agonists may be used to stop bleeding from nasal mucosa • Cardiac arrest; Epinephrine or isoprenaline may be used by IV roué or by intra-cardiac injection • They may be used in complete heart block