Download
1 / 45
450 likes | 585 Views
Use of mixed methods in the evaluation of suicide prevention strategies and interventions. Stephen Platt Qualitative research and suicide Seminar, Cardiff University, 2 July 2007. Structure of presentation. Mixed methods research Suicide in Scotland: trends and context

E N D
Use of mixed methods in the evaluation of suicide prevention strategies and interventions Stephen Platt Qualitative research and suicide Seminar, Cardiff University, 2 July 2007
Structure of presentation • Mixed methods research • Suicide in Scotland: trends and context • Choose Life strategy and action plan • Evaluation plan • Selected main findings • Selected recommendations
Mixed methods research • Adoption of a research strategy involving more than one type of research method • May be mix of qualitative and quantitative methods or mix of quantitative methods or mix of qualitative methods • Increasing use of mixed methods strategies, especially combining qualitative and quantitative approaches • Many reasons why this is occurring
Why the increasing popularity of mixed methods research? (1) • Opportunity for skills enhancement • Broadening methodological repertoire mitigates vs. “trained incapacities” (Reiss) • Encourages thinking ‘outside the box’ • Cross-national research (e.g. EU) provides increased opportunities for mixed methods research
Why the increasing popularity of mixed methods research? (2) • Fits with political currency accorded to ‘practical enquiry’ that speaks to policy/ makers and informs practice • “Whole industry” (Brannen) of mixed methods research created around evidence-based policy and in policy evaluation • Increasing emphasis upon dissemination • Researchers need to communicate in “double speak” (Brannen): technical/specialised language of research and popular language that can easily communicate findings/messages to ‘users’ • Words as important as numbers in writing up research
Misconceptions of ‘the other’ • Quantitative attitudes qualitative: • Too context specific • Selection of data to fit preconceptions • Unrepresentative samples/examples • Unwarranted claims • Qualitative attitudes quantitative: • Overly simplistic • Decontextualised • Reductionist in terms of generalisations • Failing to capture subjective meaning
Rationales underlying choice of method(s) (1) • Paradigms/philosophical assumptions • Qualitative and quantitative research seen as intrinsically different (particularly with regard to philosophical traditions) • But surveys not necessarily conducted on basis of positivist assumptions and qualitative researchers using participant observation often work in realist tradition • Micro-level emphasises subjective interpretations. Macro-level concerned with larger patterns/ trends and seeks structural explanations. But all aim to understand individuals in society. Methods need to be congruent with this quest.
Rationales underlying choice of method(s) (2) • Pragmatics • Commonplace to argue that methods should be appropriate (and subordinate) to research Q • But usually many research Qs. Some may be underpinned by realist assumptions, others by interpretevist assumptions. • And practicalities of research process may change original intention anyway, with outcomes of research taking precedence • Mixed methods believed/claimed to produce “better” outcomes than reliance on single method (pragmatic orientation linked to emphasis upon policy/practice application)
Rationales underlying choice of method(s) (3) • Politics • Political rationales for using mixed methods • Example: addressing condition of women in society requires use of large-scale quantitative data (structural) as well as in-depth qualitative data (personal experience/perspective) in order to understand/expose gendered inequalities • Crucial issue is the purpose to which methods are put rather than the methods per se
Combining methods in research process: context of justification • Stage of data analysis and interpretation • Data derived from different methods cannot be added together to produce unitary reality • Possible outcomes when methods are combined • Corroboration (‘triangulation’) (‘same’ findings from different methods) • Elaboration (one method exemplifies how findings apply in particular cases) • Complementarity (findings differ but together – synergistically – they generate insights) • Contradiction (findings from different methods conflict)
Mixed methods designs: key dimensions • Logic of enquiry: inductive (aimed at discovery) or deductive (aimed at hypothesis testing) • No one-to-one correspondence between one particular logic of enquiry and one type of method • (If mixed method approach is warranted) the ordering of methods needs to be considered: sequential or simultaneous? • How dominant is a particular method going to be (consider scarce resources)?
Examples of simultaneous designs QUAL + quan QUAN + qual QUAL + QUAL QUAL + qual Examples of sequential designs Qual QUAN QUAL quan Quan QUAL QUAN qual Qual QUAL QUAL QUAL QUAL QUAL Possible permutations of mixed methods designs
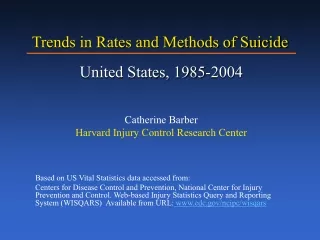
Age-standardised suicide rates, by country, 1991/93-2002/04, males
Age-standardised suicide rates, by country, 1991/93-2002/04, females
Intentional self harm & undetermined deaths, Scotland, 15+ years, 1970-2005
Scotland’s national suicide prevention strategy & action plan: Choose Life • Launched in December 2002 • Major element of Scottish Executive’s work on health improvement and mental health • Plan being implemented in phases • Budget for phase 1 (April 2003-March 2006) was £12m • Additional £8.4m allocated for first two years of phase 2 (2006-08) • Overall aim: to reduce suicide rate in Scotland by 20% in 2013 (cf 2002)
Choose Life: national and local infrastructure • Designated National Implementation Support Team (NIST) co-ordinates and supports national development and implementation • NIST’s core functions include: awareness raising/campaigning; working with the media; development/dissemination of information and knowledge; and guiding and supporting local implementation • In each local authority Choose Life action plans have been developed by the Community Planning Partnership (CPP) • National and local budgetary allocation
Evaluation: main objectives • Assess whether sustainable infrastructure is being developed nationally and locally to support achievement of Choose Life strategy • Measure and review progress towards implementation of Choose Life milestones • Examine whether and how Choose Life is stimulating effective forms of practice • Provide detailed recommendations to guide the next phase of the action plan
Theory-based evaluation • Theory-driven approaches are intended to address needs of programme implementers • Aims to articulate and test the explicit and implicit theories that shape the design and planned implementation of a programme • Attempts to determine • whether a programme has been delivered as intended • what aspects of the programme work, for whom and in what circumstances/contexts/settings • Theory of change: “a systematic and cumulative study of the links between activities, outcomes and contexts…” (Weiss)
Theory-based evaluation: the role of context • Context as a powerful ingredient in programme evolution and success – not a variable to be ‘controlled for’ • Social programmes can’t be tested/rolled out in laboratories, so getting to grips with the interface between context and intervention is of fundamental importance • Qualitative approaches can do this to a degree but rarely in a way that address concerns about programme impact
Theory-based evaluation: the process • Through a collective/collaborative process, the evaluator encourages programme stakeholders to articulate at the earliest possible stage : • The programme’s rationale • Its intended outcomes • The activities that will be implemented to achieve these • Contextual factors and their influence • The ensuing ‘theory of change’ can be used to improve programme planning and of make evaluation decisions
Main methods • Two electronic surveys of local co-ordinators • Two rounds of interviews with key informants at national level (including NIST) • Detailed and in-depth exploration of theories of change in 8 selected local areas (using interviews, workshops, observation, documentary analysis) • Two workshops with local coordinators and national informants
Co-ordinator surveys • Covering range of areas: • (Progress towards) Local vision for change • Progress in the development of the local infrastructure • Resource allocation and generation • Examples of innovative and effective practice • Monitoring and evaluation • Sustainability and mainstreaming • Collection of data on suicide and deliberate self-harm • Reflections on national support and on local progress • Open and closed questions • Rating scales to measure satisfaction with national action towards achievement of milestones and to review local implementation progress
Interviews with key informants • Key elements of semi-structured interviews: • Considering progress towards the achievement of the national milestones set out in Choose Life • Understanding the criteria applied at the national level to assess local implementation • Considering the quality of collaboration between the NIST and major national agencies for the achievement of Choose Life objectives. • Interviews with members of NIST and sample of key national informants (e.g. ChildLine, Samaritans, SAMH, NUJ) • Additional component: exploration of the NIST ‘story’ via individual interviews and joint workshop
Local area case studies (1) • Case studies were main vehicles for • exploring implementation process • identifying overall theoretical framework within which local suicide prevention teams worked • Representative sample selected by: • Geographical type (rural/remote, urban and mixed) [1º criterion] • Local suicide rate, focus on priority groups, interaction between national and local levels, and approaches to coordination [2º criteria] • Two fieldwork visits 6 months apart
Local area case studies (2) • Interviews with case study informants • Purposive sampling: 4 key informants involved in decision-making process (e.g. members Choose Life partnership responsible for priority setting) and 2 representatives involved in Choose Life funded activities • 16 project activities selected for more detailed examination (2 per case study site) • Intended to provide representative selection across Choose Life priority groups and objectives • Selection negotiated with coordinators • Interviews conducted with project representative, usually project lead/manager
Local area case studies (3) • Observational activities and collection of documentation • Observation of Choose Life events (usually partnership meetings but also training days, evaluation days and practitioner fora) • Key documents included: minutes of Choose Life partnership meetings, locality reports on progress, reports of previous needs assessment • Evaluation team aimed to understand theories of change at overall programme level as well as at project level
Local area case studies (4) • Changes to approach • Workshops replaced individual interviews with stakeholders at second fieldwork visit • Provided opportunity for joint testing of, and reflection on, local area theories of change • Local participants encouraged to assess progress towards Choose Life objectives and milestones, and how this could be demonstrated • Problems created as result of mixed levels and responsibilities of participants (e.g. strategic versus operational)
National workshops (1) • Two workshops one year apart brought together evaluation team, NIST, local coordinators and several key stakeholders • 1st workshop aimed to: • develop understanding of the different models of national and local actions and activities being put in place • explore the evolving relationship between the approaches of the centre and of local areas • identify ways in which progress could be measured.
National workshops (2) • 2nd workshop aimed to: • Review progress and learning in relation to objectives of Choose Life • Test out key themes emerging from evaluation • Identify future priorities for development, support required, measures of progress and outcome, and implications for information collection and research
Data analysis (1) • Continuous (iterative) process throughout study • Evaluation database designed and used to store (and retrieve) data on all 32 local areas • Findings from each element of data collection (case studies, workshops, national interviews, surveys) written up in detailed reports which were then used for comparative analysis • Data analysed according to predefined themes (e.g. sustainability, partnerships) … • … and themes also developed from inductive analysis conducted at each phase of evaluation
Data analysis (2) • Analytic framework developed to guide team through the evaluation • This was expanded and changed according to themes emerging from data • Analysis primarily drew on ‘charting’ method of systematically handling complex datasets by drawing out dimensions relating to each theme across all ‘cases’
Evaluation: main findings • Sustainable infrastructures for implementation • Allocation and use of resources • Innovative practice and use of evidence • Sustainability • Decision making processes and learning
Sustainable infrastructures for implementation • Demonstrable progress made by NIST • CPP successes … but not as evident in less ‘mature’ partnerships and in engaging with clinical services • Various models of local coordination developed • Preference for a dedicated (full-time) coordination post … • … but evaluation unable to demonstrate the superiority of this model
Allocation and use of resources • CPPs have attracted considerable additional investment at local level and in-kind contribution … • … but areas have not been equally successful in raising additional funding … • … and there has been unnecessary duplication of effort at local level • Choose Life has stimulated a considerable amount of activity relating to self-harm … • … but local areas have different understandings of ‘high risk’ suicidal behaviour and have adopted different responses to address the problem
Innovative practice and use of evidence • Many examples of locally defined innovative practice … • … and multiple sources of information and evidence used to inform local planning and activity … • … but research rarely used systematically
Sustainability • NIST identified several achievements in building a sustainable infrastructure for suicide prevention • At local level, most success achieved in mainstreaming training activities
Decision making processes and learning • Local stakeholder consultation: key approach to set implementation priorities • Short timescale to develop first action plan was a major challenge • National support for learning has been delivered through diverse routes • NIST has highlighted a strong commitment to evaluation … • … but a national framework for evaluation remains to be completed • In local areas different levels of priority and attention have been attached to evaluation.
Recommendations: mainstreaming at national level • Incorporate Choose Life objectives and priorities into other policy streams/initiatives • Involve clinical services in population-based suicide prevention activities • Involve national voluntary sector organisations in awareness raising and campaigning • Engage in purposive innovation to test out, evaluate, learn and implement
Recommendations: mainstreaming at local level • Using intelligence from a range of sources, as tools in planning for sustainability • Building in mechanisms to track and review progress towards objectives across policy areas • More focused targeting of action is required
Recommendations: self-harm • More consideration to be given in phase 2 to the integration of self-harm into Choose Life • The strategy should continue to encompass high risk self-harm … • … but the less ‘serious’ component of self-harm cannot be ignored
Recommendations: CPP • The CPP remains the most appropriate vehicle for developing strategy and overseeing delivery in relation to Choose Life at the local level • But its limitations should be recognised • Need to examine the necessary partnerships that have yet to be put in place • Priority should be given to establishing/building on effective links with clinical & drug/alcohol services • NIST should continue to work closely with CPPs to ensure that Choose Life budgets are fully spent on suicide prevention activities
Recommendations: central coordination body • Some type of central coordination body will continue to be required in the immediate future • Key tasks: provide national oversight, assess and support performance and ensure accountability at local level, promote learning and effective knowledge transfer, and co-ordinate action. • There should be a review of how the central coordinating function is delivered and where it is situated
Choose Life evaluation (first phase):research team University of Edinburgh Stephen Platt (RUHBC) Emma Halliday (RUHBC) Margaret Maxwell (General Practice) Scottish Development Centre for Mental Health Joanne McLean Allyson McCollam Amy Woodhouse London School of Economics Dave McDaid (Health & Social Care) Glasgow University Mhairi Mackenzie (Public Health & Health Policy) Avril Blamey (Public Health & Health Policy)