Download
1 / 23
230 likes | 297 Views
Learn about the definition, incidence, pathology, and various factors contributing to miscarriage. Explore fetal, maternal, environmental, and genetic aspects influencing pregnancy loss.

E N D
MISCARRIAGE DR. SAMAA NAZER Assistant Professor of Obstetrics & Gynecology Jeddah, Saudi Arabia
Definition Termination of pregnancy either spontaneouslly or intentionally before 20 weeks of gestation calculated from the date of onset of last menses . Alternative definition: A delivery of fetus with a weight of less than 500 g. Early: before 12 weeks Late: 12 – 20 weeks Incidence: 15% - 20% Pathology:Haemorrhage into the decidua basalis, followed by necrosis of tissues adjacent to the bleeding.
Etiology: • Fetal factors • Maternal factors Fetal factors: • More than 80% of abortions occur in the first 12 weeks of pregnancy and at least half result form chromosomal anomalies.
Aneuploid abortion approximately 50 – 60% of embryos and early fetuses that are spontaneously aborted contain chromosomal abnormalities. • 95% of chromosomal abnormalities were due to maternal gametogenesis errors and 5 percent to paternal errors. • Autosomal trisomy, monosomy x (45 x), triploidy associated with hydropic placental degeneration.
Maternal factors: I - Medical disorders and environmental condition • Infection • Mycoplasma hominis, ureaplasma, urearyticum, listeria, or toxoplasma should be specifically sought in woman with recurrent abortion • Chronic debilitating disease: celiac disease has been reported to cause both male and female infertility and recurrent abortions • Endocrine abnormalities: • Hypothyroidism, thyroid antibodies were associated with an increased incidence of abortion. • Diabetes mellitus The rate of spontaneous abortion and major congenital malformation are both increased in women with insulin dependent diabetes. It depend also on the control of DM
11-Progesterone deficiency: Luteal phase defect, due to insufficient progesterone secretion by corpus luteum I11–Nutrition: Nutrition do not appear an important cause of abortion 1V–Drug use and environmental factors Tobacco: Smoking has been linked with an increased risk for abortion
Alcohol: Both spontaneous abortion and fetal anomalies may result from fregnant alcohol used during the first 8 weeks of pregnancy Caffeine: Woman who consumed at least 5 cups of coffee per day exhibited a slight increased risk of abortion. Radiation: • Insufficient doses, radiation is a recognized abortifacient • Contraception • O.C.P. and spermicidal agent does not increase the risk • IUCD increase the risk
Environmental Toxins: • Arsenic, lead, formaldehyde, benzen and ethylene oxide are possible abortifacient • Exposure to 3 or more hours of nitrous oxide per day without gas scavenging equipment. Woman occupationally exposed to anesthetic gases had increased risk of spontaneous abortion
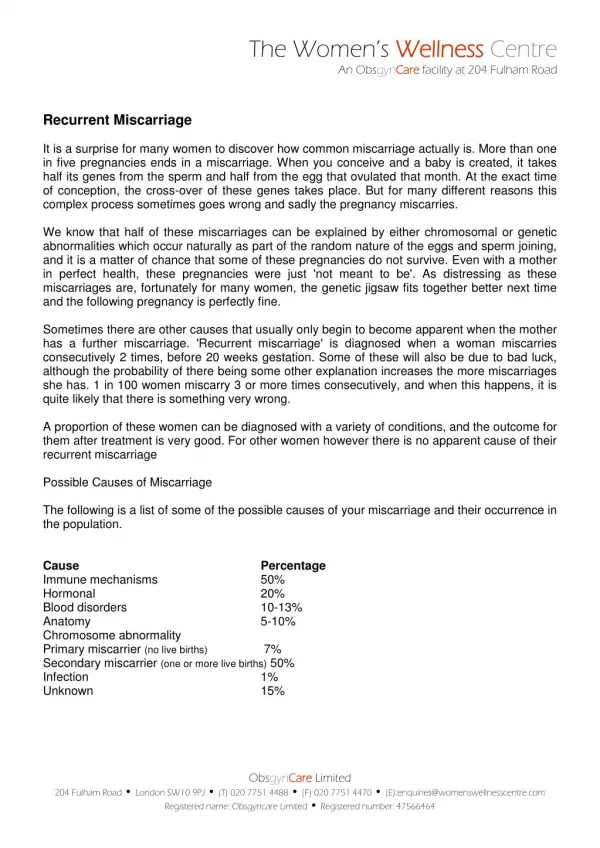
V-IMMUNOLGICAL FACTORS: • Immune system is important in recurrent pregnancy loss (15% of aborting women) Autoimmune factors: • Antiphospholipids antibodies (lupus anticoagulant, anticardiolipin antibody) • The mechanism of pregnancy loss in women with these antibodies involve placental thrombosis and infarction • Women with both history of early pregnancy loss and high level of those antibodies may suffer a 70% abortion recurrence • ALLO immune factors • Inherited thrombophilia • Several genetic disorders of blood coagulation may increase the risk of thrombosis
VI – PHYSICAL TRAUMA : In general contribute minimally to the incidence of abortion VII - Uterine defects: Acquired uterine defect : - leiomyomas, their location is more important than their size. - Asherman syndrome (uterine synechiae) due to insufficient support of pregnancy. Developmental uterine defect: Abnormal mullerian duct formation, fusion defect (spontaneously or may follow in utero-exposure to diethylstilbestrol) Incompetent cervix: • It is characterized by painless cervical dilation in the second trimester with prolapse and ballooning of membrane into the vagina followed by expulsion of an immature fetus.
Etiology of incompetant cx : • Previous trauma to the cervix (dilation and curettage, conization, cauterization, amputation) exposure to diethylstibestrol VIII - Paternal factors: • Little is known about paternal factor in the gensis of spontaneous abortion, certainly chromosomal abnormality in the sperm
Types of spontaneous abortion: 5 subgroups 1. Threatened 2. Inevitable 3.Complete or incomplete 4.Missed abortion 5.Recurrent abortion
I – Threatened abortion: Diagnosed clinically when bloody vaginal discharge or bleeding appears through a closed cervical os during the first half of pregnancy . Prognosis: 1. Half of the cases abort, the risk decrease if fetal cardiac activity can be documented 2. Increase risk of preterm delivery 3 . Increase low birth weight fetuses 4. Increase perinatal death Note: The risk of a malformed infant does not appear to be increased Treatment: • Bed rest • Anti D
II - Inevitable abortion: Bleeding, evidence of rupture of membrane and the presence of cervical dilation Treatment: • Allow abortion III - Complete, Incomplete abortion: • Complete abortion: spontaneous expulsion of the fetus and placenta from the uterine cavity • Clinically the cervix is closed • Ultrasound show empty uterus
Incomplete abortion: • Passage of some but not all fetal or placental tissue through the cervix • The diagnosis is radiological and clinical Treatment: is evacuation
IV - Missed abortion: • The uterus retains dead products of conception behind a closed cervical os for days or even weeks Diagnosis: Clinically: • Absence of pregnancy symptoms . • Size of uterus smaller than date . • Vaginal bleeding . • Radiologically.
Investigation: • CBC, PT, PTT,fibrinogen level,BhCG,pelvic us. Management: • Surgical,immediate evacuation. • Medical • Expectant (disadvantage DIC if left 3 – 5 weeks ). IV-Recurrent abortion: • The consecutive loss of three or more pregnancies before 20 weeks of gestation. Causes: • Systemic causes : diabetes mellitus ,SLE, thyroid disease, lupus anticoagulant • Paternal and maternal chromosomal abnormality. • Uterine anomalies
Investigation: • GTT • TFT • Antiphospholipid antibody,and anticardiolipin ab, ANA • Paternal chromosomal analysis • Hysterosalpingogram
American college of obstetrics and gynecology(2001) recognize two test: 1- Paternal cytogenetic analysis to identify couples at risk of unbalanced chromosomal translocation. 2 - lupus anticoagulant and anticardiolipin antibodies assay, thrombophilia antibody assay.
INDUCED ABORTION: • medical } before fetal viability • surgical } Indication: Maternal • Persistent heart disease after cardiac decompensation • Advanced hypertensive vascular disease • Invasive carcinoma of the cervix Fetal • Fetuses incompatible to life • Legal factors
CONSEQUENCES OF ELECTIVEABORTION • Maternal mortality • Impact on future pregnancies: Increase second trimester spontaneous abortion, preterm delivery, ectopic pregnancy increase risk of placenta previa. • Septic abortion: 1. criminal abortion 2. Pregnancy on top of intrauterine contraceptive device
RESUMPTION OF OVULATION AFTER ABORTION: Ovulation may resume as early as 2 weeks after an abortion Differential diagnosis of bleeding in early pregnancy • Abortion • Ectopic pregnancy • Vesicular mole • Endometrial carcinoma • Cervical polyp • Cervical lesion and erosion • Trauma • Medical disease (coagulation defect)