Download
1 / 6

E N D
0889-8529/99 $8.00 + .OO HYPOGLYCEMIC DISORDERS SYMPTOMS OF HYPOGLYCEMIA, THRESHOLDS FOR THEIR OCCURRENCE, AND HYPOGLYCEMIA UNAWARENESS Philip E. Cryer, MD Decreasing plasma glucose concentrations normally elicit a typical sequence of responses8 (Table 1). Insulin secretion decreases as plasma glucose levels fall within the physiologic range. Secretion of glucose counterregulatory hormones (glucagon, epinephrine, cortisol, and growth hormone) increases as plasma glucose levels fall just below the physio- logic range. Symptoms are perceived at lower plasma glucose levels; even lower plasma glucose levels cause cognitive dysfunction seizures, loss of consciousness, and, ultimately, death. SYMPTOMS OF HYPOGLYCEMIA Although they are often typical, symptoms of hypoglycemia are nonspecific. Symptoms can be confidently attributed to hypoglycemia only when Whipple's triad is fulfilled, that is, the symptoms are consis- tent with 'hypoglycemia, a low plasma glucose concentration is present, This work was supported, in part, by National Institutes of Health grants RO1 DK27085, M01 RR00036, P60 DK20579, and T32 DK07120 and by a fellowship award from the American Diabetes Association. From the Division of Endocrinology, Diabetes, and Metabolism, Washington University School of Medicine, St. Louis, Missouri ENDOCRINOLOGY AND METABOLISM CLINICS OF NORTH AMERICA ~~ 495 VOLUME 28 * NUMBER 3 SEPTEMBER 1999
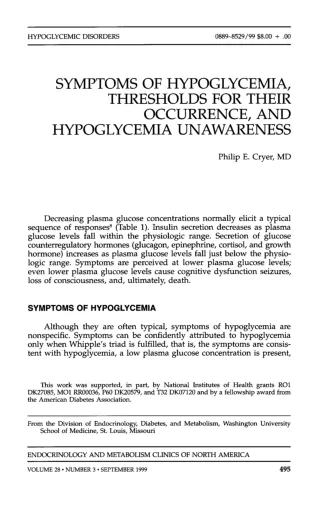
496 CRYER Table 1. SEQUENCE OF, AND ARTERIALIZED VENOUS GLYCEMIC THRESHOLDS FOR, RESPONSES TO FALLING PLASMA GLUCOSE CONCENTRATIONS Response Threshold 1. Decreased insulin secretion 2. Increased glucagon, epinephrine, cortisol, and growth hormone secretion -80 mg/dL -65 mg/dL -55 mg/dL -45 mg/dL 3. Symptoms 4. Cognitive dysfunction Datafrom references 11, 19, and 21. and the symptoms are relieved after the plasma glucose level is raised to or above normal. Symptoms of hypoglycemia are ultimately traceable to neuronal glucose deprivation and can be divided into two categories: neurogenic (or autonomic) and neuroglycopenic symptomss, 23 (Fig. 1). Neurogenic symptoms are the result of the perception of physiologic changes caused by the autonomic nervous system discharge triggered by hypogly~emia.~~ Adrenergic (catecholamine-mediated) symptoms in- clude tremulousness, palpitations, and anxiety. The extent to which these symptoms are mediated by norepinephrine released from sympathetic postganglionic nerve terminals within the target tissues, epinephrine released from the adrenal medullae into the circulation, or both is not Tingling S haky1Tremulous Heart pounding NervousIAnxious Difficulty thinking/ Confused lired/Drowsy Faint Dizzy Difficulty speaking Blurred vision + 2 - 1 - - 0 - Figure 1. Neurogenic (autonomic) and neuroglycopenic symptoms of hypoglycemia. Mean (k SE) scores for awareness of hypoglycemia (“blood sugar low”) recorded by the subjects during euglycemia (EU) and hypoglycemia (HYPO) alone (solid bar), with combined a- and p-adrenergic blockade with phentolamine and propranolol (ADB, crosshatched bar) and with panautonomic blockade with phentolamine, propranolol, and atropine (PAB, shaded bar) are also shown. (Data from Towler DA, Havlin CE, Craft S, et al. Mechanism of awareness of hypoglycemia. Perception of neurogenic (predominantly cholinergic) rather than neuroglycopenic symptoms. Diabetes 42:1791, 1993; figure from Cryer PE: Hypogly- cemia: The limiting factor in the management of IDDM. Diabetes 43:1378, 1994; with permission.)
497 SYMPTOMS OF HYPOGLYCEMIA AND HYPOGLYCEMIA UNAWARENESS entirely clear; however, tremor has been attributed to sympathetic neural activation and palpitations to adrenomedullary a~tivation.'~, ergic (acetylcholine-mediated) symptoms include sweating, hunger, and paresthesias. At least the diaphoretic response is thought to be mediated by sympathetic cholinergic postganglionic neurons.6, l5 Neuroglycopenic symptoms are the result of brain glucose depriva- tion, per se. They include difficulty in thinking or confusion and sensa- tions of warmth, weakness, and fatigue,u as well as more severe cogni- tive failure, behavioral changes, seizures, coma, and, ultimately, death. All of the symptoms of hypoglycemia, including the neurogenic symp- toms, are fundamentally neuroglycopenic in origin. Symptoms of hypoglycemia reported by patients with insulinomasZ are listed in Table 2. 15, l6 Cholin- GLYCEMIC THRESHOLDS The hyperinsulinemic stepped hypoglycemic clamp technique has been used to quantitate arterialized venous glycemic thresholds for the various responses to falling plasma glucose concentrations.11, Representative values are shown in Table 1. With that technique, the glycemic threshold is defined as the plasma glucose concentration at which a given parameter first deviates from the 95% confidence interval for that parameter at the same time point during hyperinsulinemic euglycemic clamps in the same individuals. A variety of other ap- proaches to the estimation of glycemic thresholds (typically significant deviations from baseline values) have been used. Although these esti- mated thresholds can be useful for within study comparisons, they cannot be extrapolated to the thresholds determined from paired stepped hypoglycemic and euglycemic clamps. When this technique is used, the glycemic thresholds for the various responses to falling plasma glucose concentrations are generally repro- ducible from laboratory to laboratory.*, 11, 19, 21 Nonetheless, the glycemic thresholds are dynamic rather than static. They shift to higher plasma glucose concentrations following sustained hyperglycemia (e.g., in per- sons with poorly controlled diabetes mellitus)', and to lower plasma 19, 21 Table 2. SYMPTOMS OF HYPOGLYCEMIA IN PATIENTS WITH INSULINOMAS Symptoms Incidence Various combinations of diplopia, blurred vision, sweating, palpitations, or weakness 85% Confusion or abnormal behavior Unconsciousness or amnesia Generalized convulsions 80% 53% 12% Data from Service FJ, Dale AJD, Elveback LR, et al: Insulinoma: Clinical and diagnostic features of 60 consecutive cases. Mayo Clinic Proc 51:417,1996.
490 CRYER glucose concentrations following episodes of hypoglycemia (e.g., in fre- quently hypoglycemic persons with tightly controlled diabetes mellitus' or those with hypoglycemia caused by an in~ulinoma'~). are undoubtedly the result of previous hypoglycemia? l4 the precise mechanisms of these shifts in glycemic thresholds are not known. Changes in the rate of blood-to-brain glucose transport at a given plasma glucose concentration have been proposed.8 Preserved brain glucose uptake as determined with the Kety-Schmidt technique (the product of the arteriovenous glucose difference across the brain and brain blood flow) has been reported in healthy subjects following 56 hours of hypo- glycemia3 and in persons with tightly controlled type 1 diabetes4 Although they HYPOGLYCEMIA UNAWARENESS Recognized since the initial experience with insulin to treat diabetes in the 1920s; hypoglycemia unawareness is loss of the warning, almost exclusively neurogenic symptoms of developing hypoglycemia that pre- viously prompted the individual to act (e.g., eat) to abort the episode. It is a reflection of shifts of glycemic thresholds for the autonomic nervous system response that cause neurogenic symptoms to lower plasma glu- cose concentrations perilously close to levels that cause cognitive failure. When plasma glucose levels fall low enough to trigger a substantial autonomic response, the patient may not be able to perceive or interpret the resultant physiologic changes as indicative of hypoglycemia because of impaired cerebral function. As a result, an episode of severe clinical hypoglycemia ensues. The magnitude of the responses, including the symptomatic re- sponses, to low plasma glucose levels is a function of the nadir plasma glucose concentration rather than the rate or magnitude of the The clinical observation that patients with tightly controlled diabetes or insulinomas often tolerate relatively low plasma glucose concentrations without noticeable symptoms (i.e., that they exhibit hypoglycemia un- awareness) is not attributable to gradual reductions in the plasma glu- cose levels. Rather, this observation is attributable to the ability of previous hypoglycemia to shift the glycemic threshold for symptoms to a lower plasma glucose concentration. Hypoglycemia unawareness can be induced by prior hypoglycemia in healthy or patients with diabetes9 and can develop in persons with ins~linomas.~~ It can be reversed by scrupulous avoidance of iatrogenic hypoglycemia in patients with diabetes7* elimination of hypoglycemia following surgical treatment of insulino- mas.17 18, *O lo, l2 and by the ACKNOWLEDGMENTS The author acknowledges the substantive contributions of his colleagues whose names appear i n the list of references and the assistance of Karen Muehlhauser i n the preparation of this manuscript.
499 SYMPTOMS OF HYPOGLYCEMIA AND HYPOGLYCEMIA UNAWARENESS References 1. h i e l SA, Sherwin RS, Simonson DC, et al: Effect of intensive insulin therapy on glycemic thresholds for counterregulatory hormone release. Diabetes 37901, 1988 2. Amiel SA, Simonson DC, Tamborlane WV, et al: Rate of glucose fall does not affect counterregulatory hormone responses to hypoglycemia in normal and diabetic hu- mans. Diabetes 36518, 1987 3. Boyle PJ, Nagy R, OConner AM, et al: Adaptation in brain glucose uptake following recurrent hypoglycemia. Proc Natl Acad Sci USA 91:9352, 1994 4. Boyle PJ, Kempers SF, OConner AM, et al: Brain glucose uptake and unawareness of hypoglycemia in patients with insulin dependent diabetes mellitus. N Engl J Med 333:1726, 1995 5. Boyle PJ, Schwartz NS, Shah SD, et a1 Plasma glucose concentrations at the onset of hypoglycemic symptoms in patients with poorly controlled diabetes and in nondiabet- ics. N Engl J Med 318:1487, 1988 6. Chalmers TM, Keele C H The nervous and chemical control of sweating. Br J Dermatol 64:43, 1952 7. Cranston I, Lomas J, Maran A, et al: Restoration of hypoglycemia unawareness in patients with long duration insulin-dependent diabetes mellitus. Lancet 344:283, 1994 8. Cryer PE: Hypoglycemia: Pathophysiology, Diagnosis and Treatment. New York, Ox- ford University Press, 1997 9. Dagogo-Jack S, Craft S, Cryer PE: Hypoglycemia-associated autonomic failure in insu- lin dependent diabetes mellitus. J Clin Invest 91:819, 1993 10. Dagogo-Jack S, Rattarasarn C, Cryer PE: Reversal of hypoglycemia unawareness, but not defective glucose counterregulation, in IDDM. Diabetes 43:1426, 1994 11. Fanelli C, Pampanelli S, Epifano L, et al: Relative roles of insulin and hypoglycaemia on induction of neuroendocrine responses to, symptoms of, and deterioration of cognitive function in hypoglycaemia in male and female humans. Diabetologia 37797, 1994 12. Fanelli C, Pampanelli S, Epifano L, et al: Long-term recovery from unawareness, deficient counterregulation, and lack of cognitive dysfunction during hypoglycemia following institution of rational intensive therapy in IDDM. Diabetologia 371265,1994 13. French EB, Kilpatrick R The role of adrenaline in hypoglycaemic reactions in man. Clin Sci 14639, 1955 14. Heller SA, Cryer PE: Reduced neuroendocrine and symptomatic response to subse- quent hypoglycemia after one episode of hypoglycemia in nondiabetic humans. Diabe- tes 40223, 1991 15. Heller SR, Macdonald LA: Physiological disturbance in hypoglycaemia: Effect on sub- jective awareness. Clin Sci 81:1, 1991 16. Kerr D, Macdonald IA, Heller SR, et al: A randomized double blind placebo controlled trial of the effects of metoprolol CR, atenolol and propranolol LA on the physiological responses to hypoglycemia in nondiabetic subjects. Br J Clin Pharmacol29:685, 1990 17. Mitrakou A, Fanelli C, Veneman T, et a1 Reversibility of hypoglycemia unawareness. N Engl J Med 329:834, 1993 18. Mitrakou A, Mokan M, Ryan C, et al: Influence of plasma glucose rate of decrease on hierarchy of responses to hypoglycemia. J Clin Endocrinol Metab 76:462,1993 19. Mitrakou A, Ryan C, Veneman T, et al: Hierarchy of glycemic thresholds for counter- regulatory hormone secretion, symptoms and cerebral dysfunction. Am J Physiol 260:E67, 1991 20. Santiago JV, Clarke WL, Shah SD, et al: Epinephrine, norepinephrine, glucagon, and growth hormone release in association with physiological decrements in the plasma glucose concentration in normal and diabetic man. J Clin Endocrinol Metab 51:877,1980 21. Schwartz NS, Clutter WE, Shah SD, et al: Glycemic thresholds for activation of glucose counterregulatory systems are higher than the threshold for symptoms. J C h Invest 79777, 1987 22. Service FJ, Dale Am, Elveback LR, et al: Insulinoma: Clinical and diagnostic features of 60 consecutive cases. Mayo Clinic Proc 51:417, 1976
500 CRYER 23. Towler DA, Havlin CE, Craft S, et al: Mechanisms of awareness of hypoglycemia: Perception of neurogenic (predominantly cholinergic) rather than neuroglycopenic symptoms. Diabetes 421791, 1993 Address reprint requests to Philip E. Cryer, MD Division of Endocrinology, Diabetes and Metabolism Washington University School of Medicine Campus Box 8127 660 South Euclid Avenue St. Louis, MO 63110 e-mail: pcryerQimgate.wustl.edu