Download
1 / 42
901 likes | 2.56k Views
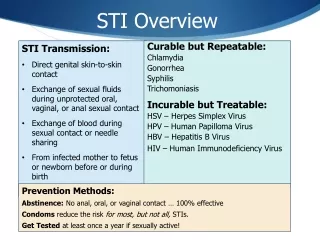
Syndromic Management of STI. John Q. Wong, MD, MSc 20 November 2010. STI Case Management. History-taking and examination Diagnosis and treatment, using flowcharts Counseling and education on safer sex, including condom promotion and provision Partner management

E N D
Syndromic Management of STI John Q. Wong, MD, MSc 20 November 2010
STI Case Management • History-taking and examination • Diagnosis and treatment, using flowcharts • Counseling and education on safer sex, including condom promotion and provision • Partner management • Data gathering (recording)
Traditional approaches to STI diagnosis • Etiological diagnosis • Lab tests to identify the causative agent • Clinical diagnosis • Clinical experience to identify symptoms typical for a specific STI
Etiological approach • Treatment has to wait for lab results • Testing facilities not available • Lab tests not ideal for some STIs • H. ducreyi not easily cultured • C. trachomatis tests are expensive and invasive • Syphilis requires a special microscope and training
Clinical diagnosis • Some STIs cause similar symptoms • Mixed infections are common
The third way: syndromic case management • Problem-oriented (patient’s symptoms) • Highly sensitive and does not miss mixed infections • Treats the patient at the first visit • Makes STI care more accessible (primary care level) • Uses flowcharts • Provides opportunity and time for education and counseling
Criticisms of the syndromic approach • Not scientific • Studies have shown similar diagnostic accuracy as clinical diagnosis, except for syphilis • Tanzania used syndromic approach in 1995 trial • 50% reduction in urethritis in men • Reduction in syphilis • 38% reduction in HIV
Criticisms of the syndromic approach • Too simple for a physician - can even be used by nurses • Just like thermometers and stethoscopes • Use by other service providers also an advantage • More time for education for behavior change
Criticisms of the syndromic approach • Fails to make use of a service provider’s clinical skills and experience • Studies have shown that clinicians using their own clinical judgment misdiagnose 50% of the time • Treat patient for the most common cause, then treat for a second cause if symptoms do not improve • Most patients do not return to the health center • Patient will continue to transmit the STI
Criticisms of the syndromic approach • Results in waste of drugs because patients are being over-treated • Studies have shown that syndromic approach is less expensive • Gram stain should be included in STI diagnosis • Delay in treatment • Costly • Quality assurance required
This shape indicates the client’s presenting complaints Every flow chart will start with this shape – it has one exit only Clients complains of … This shape indicates an instruction : do this! e.g., examine the client It has one entry arrow and one exit arrow This shape indicates a question No It has one entry arrow and two exits – a ‘yes’ exit and a ‘no’ exit e.g., is there a discharge? Yes Syndromic Case Management Flow Chart 1. 2. 3.
Patient complains of urethral discharge and/or burning Discharge present ? No 7 days Symptom persist? Yes Urethral Discharge Take medical and sexual history; milk urethra if necessary Reassure 2Cs 4 Cs Counseling, Condom, Compliance, Contact Tracing 3 Cs Counseling, Condoms, Compliance 2 Cs Counseling, Condoms Yes Treat for Discharge (Gonorrhea/Chlamydia) 4 Cs Refer
Treatment Guidelines • For Gonorrhea (gonococcal urethritis/cervicitis) • Cefixime 400 mg. Orally single dose OR • Ceftriaxone 250 mg. IM single dose PLUS • Treatment for non-gonococcal urethritis or cervicitis • For Chlamydia (non-gonococcal urethritis/cervicitis) • Azithromycin 1 gram Orally single dose OR • Doxycycline 100 mg. Orally 2x a day for 7 days • Tetracycline 500 mg. Orally 4x a day for 7 days • If Pregnant: • Erythromycin 500 mg. Orally 4x a day for 7 days
Patient with vaginal discharge A C B Take History Sexual partner with urethral discharge in past 3 month? Review history Examine with speculum No D G Yes No One clinical and one behavioral positive? (Risk factor) Treat for vaginitis 3 Cs Treat for cervicitis Treat for vaginitis 4 Cs Yes Vaginal Discharge E F 4 Cs Counseling, Condom, Compliance, Contact Tracing 3 Cs Counseling, Condoms, Compliance 2 Cs Counseling, Condoms Note: if symptoms persist after treatment: REFER
Risk factors for vaginal discharge • being under 21 years of age (or 25 in some settings); • being unmarried; • having more than one sexual partner in the last three months; • having a new partner in the last three months; • the current partner having a sexually transmitted infection; • recent use of condoms by the partner.
A B E Sexual partner with urethral discharge in past 3 mos.? No No M One clinical & one behavioral positive? No D No Budding yeast or pseudohyphae present? Yes Whiff test positive? Yes Yes Yes J L P No Whiff test positive? No Budding yeast or pseudohyphae present? Treat for cervicitis 2 Cs G Yes O Yes Q Vaginal Discharge(if with laboratory support (microscope, KOH 10% & trained health care workers) & facilities for genital examination) Patient with vaginal discharge Take History Review history Examine with speculum Whiff test and wet mount Resume 2 Cs Treat for cervicitis Treat for vaginitis 4 CS Treat for candidiasis 2 Cs Treat for TV/BV 4 Cs 4 Cs Counseling, Condom, Compliance, Contact Tracing 3 Cs Counseling, Condoms, Compliance 2 Cs Counseling, Condoms Treat for cervicitis Treat for candidiasis 4 CS Treat for cervicitis Treat for TV/BV 4 CS *TV: Trichomonas vaginalis BV: Bacterial vaginosis
Treatment Guidelines • For Gonorrhea (gonococcal urethritis/cervicitis) • Cefixime 400 mg. Orally single dose OR • Ceftriaxone 250 mg. IM single dose PLUS • Treatment for non-gonococcal urethritis or cervicitis • For Chlamydia (non-gonococcal urethritis/cervicitis) • Azithromycin 1 gram, Orally single dose OR • Doxycycline 100 mg. Orally 2x a day for 7 days OR • Tetracycline 500 mg. Orally 4x a day for 7 days • If Pregnant • Erythromycin 500 mg. Orally 4x a day for 7 days
Treatment Guidelines • For Trichomoniasis • Metronidazole 2 grams Orally single dose • Metronidazole 500 mg. Orally 2x a day for 7 days • NOTE: Do not use in the first trimester of pregnancy, for symptomatic relief: Clotrimazole 100 mg. Vaginal Suppository for 7 days
Treatment Guidelines • For Bacterial Vaginosis • Metronidazole 500 mg. Orally 2x a day for 7 days OR • Metronidazole 2 grams, Orally single dose • NOTE:First trimester of pregnancy: Clindamycin 300 mg. Orally 2x a day for 7 days • For Candidiasis • Clotrimazole 500 mg. Per vagina single dose OR • Miconazole 400 mg. Per vagina each night for 3 days
Patient complaining of genital sore(s) B H No A single ulcer? Start as vesicular lesions and recurrent in same place No Yes Yes Treat for herpes symptomatic relief Reassure 4 C’s I D No Treat for syphilis 4 C’s See 1 week K Painful? Yes L No Resolving? Yes F No Resolving? Yes Genital Ulcer Take history and examine Reassure 2 C’s Refer 1.Treat for herpes 2.Symptomatic relief 3.Reassure 4 Cs 4 Cs Counseling, Condom, Compliance, Contact Tracing 3 Cs Counseling, Condoms, Compliance 2 Cs Counseling, Condoms 4 C’s Refer 4 C’s
Treatment Guidelines • For Primary Genital Herpes • Acyclovir 400 mg. Orally 3x a day for 10 days OR • Valaciclovir 1000 mg. Orally 2x a day for 10 days • For Secondary Genital Herpes • Acyclovir 400 mg. Orally 3x a day for 5 days OR • Valaciclovir 500 mg. Orally 2x a day for 5 days
Treatment Guidelines • For Syphilis: Early Syphilis (Primary, Secondary, Early Latent <2 years) • Benzathine Penicillin G 2.4 M units IM single dose • If allergic to Penicillin: • Doxycycline 200 mg Orally 2x a day for 14 days OR • Tetracycline 500 mg. Orally 4x a day for 14 days • If allergic to Penicillin and Pregnant: • Ceftriaxone 250 mg. IM every other day for 5 doses
Treatment Guidelines • Late Syphilis (Late Latent >2 years) • Benzathine Penicillin G 2.4 M units IM weekly for 3 doses for a total of 7.2 M units • If allergic to Penicillin: • Doxycycline 200 mg. Orally 2x a day for 4 weeks OR • Tetracycline 500 mg. Orally 4x a day for 4 weeks • If allergic to Penicillin and Pregnant: • Ceftriaxone 250 mg. IM every other day for 10 doses
Patient complains of Scrotal Swelling / Pain F Swelling/ tenderness confirmed? Reassure 2 C’s No Yes No G D Treat for gonorrhea Treat for chlamydia 4 Cs Advise support to scrotum Return in 5-6 days History of trauma? Testis rotated or elevated? Yes No E Improving? Refer to Surgeon Immediately Yes Scrotal Swelling Take history and examine Refer 4 Cs Counseling, Condom, Compliance, Contact Tracing 3 Cs Counseling, Condoms, Compliance 2 Cs Counseling, Condoms Complete remaining treatment 4 C’s
Treatment Guidelines • For Gonorrhea (gonococcal urethritis/cervicitis) • Cefixime 400 mg. Orally single dose OR • Ceftriaxone 250 mg. IM single dose PLUS • Treatment for non-gonococcal urethritis or cervicitis • For Chlamydia (non-gonococcal urethritis or cervicitis) • Azithromycin 1 gram Orally single dose OR • Doxycycline 100 mg. Orally 2x a day for 7 days OR • Tetracycline 500 mg. Orally 4x a day for 7 days
Patient complains of lower abdominal pain A Fever >38? And/or pain on moving cervix? And/or vaginal discharge Missed or overdue periods? And/or recent delivery abortion? And/or Abdominal guarding? And/or Rebound tenderness? And/or Vaginal bleeding? And/or Palpable, painful masses? C E No No Yes Treat for PID 4 Cs Follow-up in 3-7 days depending on severity F Yes G No Improving? Yes Lower abdominal pain in women 4 Cs Counseling, Condom, Compliance, Contact Tracing 3 Cs Counseling, Condoms, Compliance 2 Cs Counseling, Condoms Take history Examine abdomen Do speculum examination Do bimanual examination Follow up if pain persist Refer to Surgeon Immediately Refer Continue treatment to complete 14 days
Treatment Guidelines • For Pelvic Inflammatory Disease • * Single dose treatment for gonorrhea) • Cefixime 400 mg. Orally OR Ceftriaxone 250 mg. IM PLUS • * Treatment for chlamydial infection for 14 days • Doxycycline 100 mg. Orally 2x a day OR • Tetracycline 500 mg. Orally 4x a day PLUS • * Treatment for anaerobic infection for 14 days • Metronidazole 500 mg. Orally 2x a day
Newborn presents with discharge from the eye (s) One or both eyes swollen? discharge from one or both eyes? One or both eyes swollen? Discharge from one or both eyes? No No Yes Yes swelling & discharge greatly improved Yes Yes Newborn conjunctivitis Take medical and sexual history from mother and examine infant Reassure but review in 3 days Reassure • Treat newborn for gonococcal and chlamydial infection (Ophthalmia Neonatorum) • Treat mother and partner for gonorrhea and chlamydial infection • 4 Cs, including other safer sex alternatives • Client chooses most practical option practice negotiation with clients review in 3-7 days 4 Cs Counseling, Condom, Compliance, Contact Tracing 3 Cs Counseling, Condoms, Compliance 2 Cs Counseling, Condoms Complete remaining treatment 4 Cs, including other safer sex alternatives Client chooses most practical option practice negotiation with clients *careful priming (what kind of questions, why, and how will it help in the counseling) *assurance of confidentiality
Treatment Guidelines • For Ophthalmia Neonatorum • Ceftriaxone 25-50 mg./kg. BW IM single dose, to a max. of 125 mg. PLUS • Erythromycin 50 mg./kg. BW per day in 4 divided doses for 14 days
Case Study #1 • A patient complains of a discharge from the penis. Upon examination, you notice a discharge from the urethra. • What is the syndrome?
Case Study #2 • A young woman complains of a sore. Upon examination you notice an ulcer on the outer labia. • What is the syndrome?
Mas is an adolescent boy of 15 years who lives in the slum area of a large town. He has been brought to the district hospital because his scrotum is swollen and he is vomiting. What flowchart do you use? On examination, the scrotum is swollen and painful; the testes elevated and rotated. How do you manage this patient? Case Study #3
Case Study #4 • Gloria took her four-day-old baby to the clinic when she noticed that his right eye was swollen and there was pus in both eyes (the right eye more than the left). • What flowchart do you use? • What treatment do you offer, to whom?
Case Study #5 • Doris, aged 22, attended the family planning clinic for her usual check-up while on the contraceptive pill. She tells the nurse about a yellow, itchy vaginal discharge that she has had for the past four days. • What flowchart do you use?
Case Study #5 • Doris says she has no abdominal pain or urination pain. She had her period two weeks ago and it was normal. Shyly, she discloses that she had sex with an old school friend a week ago, and that she did not use a condom because she was on the pill. She last had sex with her regular boyfriend a month ago, as he was out of town. • For what do you treat Doris?