Download
1 / 21
210 likes | 429 Views
The Global Epidemiology of HIV among Female Sex Workers: The Influence of Structural Determinants Shannon K, Strathdee SA , Goldenberg S, Duff P, Mwangi P, Reza-Paul S, Rusakova M, Lau J, Deering K, Pickles M, Boily MC. HIV Burden among Female Sex Workers (FSWs) .

E N D
The Global Epidemiology of HIV among Female Sex Workers: The Influence of Structural DeterminantsShannon K, Strathdee SA, Goldenberg S, Duff P, Mwangi P, Reza-Paul S, Rusakova M, Lau J, Deering K, Pickles M, Boily MC
HIV Burden among Female Sex Workers (FSWs) • FSWs bear a disproportionate burden of HIV worldwide • 13.5 times more likely to be HIV positive than general population* • Despite decades of research and program activity, the epidemiology of HIV and structural determinants in sex work remain poorly understood • Behavioural and biomedical interventions alone have had only modest impact,leading to calls for combination HIV prevention, including structural and community-led efforts • *Baral et al, Lancet 2013
Overview of Methods • Systematic review of available epidemiological data on HIV and female sex work • Review role of structural determinants in HIV epidemics among FSWs and gaps in data • Deterministic transmission dynamic models to determine the prevention potential of structural interventions to avert HIV infections in 3 settings (Kenya, India, Canada) with different epidemic settings and history of interventions • Key structural factors modeled based on context-specific epidemiological, qualitative and grey literature
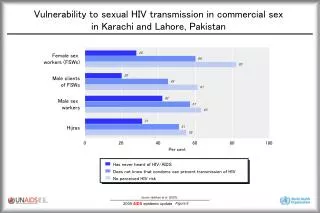
All published studies 2008-2013 including HIV (HIV/STI) or condom use outcomes • Majority of studies from LMIC (93%), data disproportionately drawn from Asia • Large gaps in science from high HIV burden regions (e.g. Sub-Saharan Africa, Russia, E. Europe) • <50% of published studies explicitly examined structural determinants • Yet broader literature underscores the centrality of structural determinants for this component of the global HIV epidemic Systematic Review:State of HIV Epidemiology in Female Sex Work
HIV • Criminalized and punitive laws & policies • Law enforcement strategies & local policing • Demolition/gentrification of red light districts Macro-Structural Determinantsthat promote HIV risk among FSWs “You know, you get these asshole cops and security kicking us off and moving us to darker and darker areas. This has to stop” -Sex Workers, Vancouver (Shannon et al, 2008)
Macro-Structural Determinantsthat promote HIV risk among FSWs • HIV risk • Suboptimal access to safe, appropriate sexual health care, condoms, HIV/ STI testing, ART “When I fell sick and went to a health centre and they realised that I was a sex worker, they did not treat me like a human being […] I was told that he had no time for me. So I left without getting treatment.” -Sex Worker, Mombasa, Kenya (Scorgie et al., 2013)
HIV • Supportive work environments • Community empowerment Sex Work Environments thatReduce HIV Risk among FSWs • “I hear and see mistreatment • of sex workers by clients • but I throw them out. • I call the police patrol too, • the mobile jeep, • and get the client out” • -Transgender Woman Sex Worker/ Lodge Owner, • Karnataka, India • (Argento, Reza-Paul, et al., 2011)
Structural factors = Work environment Vancouver: Injection drug use (risk) Kenya : Binge drinking(risk) India: Sex work collective (risk) Dynamic Pathways for Structural Factors & HIV Acquisition/ Transmission in Female Sex Work • PWID : Person who injects drugs • IRR: relative incidence ratio of experiencing violence • RRc >1 Relative risk of inconsistent condom use (ICU) following this experience of violence
Included in model (based on available data) Vancouver: Recent and non recent history of police harassment and client sexual or physical violence Kenya : Recent workplace sexual violence India: Recent workplace physical/sexual violence and fear of condom confiscation Dynamic Pathways for Structural Factors & HIV Acquisition/ Transmission in Female Sex Work • PWID : Person who inject drug • IRR: relative incidence ratio of experiencing violence • RRc >1 Relative risk of inconsistent condom use (ICU) following this experience of violence
Fraction of new HIV infections averted among FSWs and clients over ten years Modest impact due to sustained negative effects of past exposure to client sexual violence Vancouver, Canada: Potential HIV Infections Averted through Structural Change • ICU: Inconsistent condom use
Fraction of new HIV infections averted among FSWs and clients over ten years Modest impact due to combined, frequent and iterative effects of client physical violence and police harassment Vancouver, Canada: Potential HIV Infections Averted through Structural Change • ICU: Inconsistent condom use
Fraction of new HIV infections averted among FSWs and clients over ten years Vancouver, Canada: Potential HIV Infections Averted through Structural Change • ICU: Inconsistent condom use
Fraction of new HIV infections averted among FSWs and clients over ten years Vancouver, Canada: Potential HIV Infections Averted through Structural Change • ICU: Inconsistent condom use
Fraction of new HIV infections averted among FSWs and clients over ten years • Mombasa, Kenya: • Potential HIV Infections Averted through Structural Change
Fraction of new HIV infections averted among FSWs and clients over ten years • Mombasa, Kenya: • Potential HIV Infections Averted through Structural Change
Fraction of new HIV infections averted among FSWs and clients over ten years • Mombasa, Kenya: • Potential HIV Infections Averted through Structural Change
Fraction of new HIV infections averted among FSWs and clients over ten years • Mombasa, Kenya: • Potential HIV Infections Averted through Structural Change
Fraction of new HIV infections averted among FSWs and clients over ten years Bellary, India: Potential HIV Infections Averted through Structural Change
Policy & Program Implications • Critical need for structural change to have major impact on HIV response in sex work = decriminalization of sex work; elimination of violence, police harassment; safer work environments • Major gaps in coverage and equitable access to HIV prevention and treatment for FSWs (and dearth of data) – scale-up must occur in tandem with structural change and SW-led efforts • Need research to better disentangle complex, dynamic and context-specific pathways of structural determinants
Elimination of sexual violence alone due to immediate and sustained impact could avert 17-20% of HIV infections over next decade • In heavy HIV burden settings (Mombasa Kenya): • Scale-up of ART to meet WHO guidelines for both FSWs and clients could avert 34% of HIV infections over next decade • Even modest scale up of SW-led outreach could avert 20% of HIV • Decriminalization of sex work could have the largest impact on the course of HIV epidemics across all 3 settings averting 33-46% of incident HIV infections over next decade among FSWs and clients • Findings confirm calls for multi-pronged structural and community-led interventions, alongside biomedical, to reduce HIV burden and promote human rights for SWs globally Key Messages
International Co-Author Team – affiliations: • Gender & Sexual Health Initiative, BC Centre for Excellence in HIV/AIDS; University of British Columbia, Canada • University of California San Diego School of Medicine, United States • Bar Hostesses Empowerment and Support Program, African Sex Workers Alliance, Kenya • Stellit NGO, Russia • Ashodaya Samathi Collective, India • Chinese University of Hong Kong, China • Imperial College London, United Kingdom • Funding: • This work was directly supported through partial funds from UNFPA, Bill and Melinda Gates Foundation & NIH NIDA (R01DA028648; PI: Shannon) for assistance with modeling, analysis and planning meetings in London and Vancouver. S. Strathdee is supported by a NIDA MERIT award (R37 DA019829). Acknowledgements