MATERNAL COLLAPSE
NWAC. MATERNAL COLLAPSE. Berrin Gunaydin, MD, PhD Department of Anesthesiology Gazi University School of Medicine Ankara, Turkey. Discuss the incidence and causes of cardiac arrest/maternal collapse in pregnancy the physiological changes in pregnancy that make women susceptible

MATERNAL COLLAPSE
E N D
Presentation Transcript
NWAC MATERNAL COLLAPSE Berrin Gunaydin, MD, PhD Department of Anesthesiology Gazi University School of Medicine Ankara, Turkey
Discuss the incidence and causes of cardiac arrest/maternal collapse in pregnancy the physiological changes in pregnancy that make women susceptible resusciation techniques and management of cardiac arrest in pregnancy amniotic fluid embolism perimortem cesarean section NWAC OBJECTIVES
Cardiac arrest is a very rare maternity emergency (1/30000 pregnancy) It usually occurs as a result of other maternity emergencies If managed well, up to 50% of maternal deaths are preventable Many maternal deaths occur from potentially treatable causes NWAC Maternal mortality
Increased plasma volume (50%) Increased cardiac output (40%) Increased heart rate (15-20 bpm) Increased respiratory rate Increased oxygen consumption (20%) Decreased blood pressure Decreased residual lung capacity Laryngeal oedema Aoto-caval compression NWAC Physiology of Pregnancy I
Increased clotting factors Increased breast tissue Diaphragm rises by about 7 cm and the organs move for growing uterus Gut peristaltis slows NWAC Physiology of Pregnancy II
Improve blood supply for fetal nutrition Promote breast development in preparation for neonatal feeding Alter the internal organ displacement to make room for the growing fetus and uterus NWAC Major body changes for the pregnant woman
Oestrogen Increased excitability in uterine muscle fibers Increased susceptibility to catecholamines Progesterone İncreased tidal volume and respiratory rate Hyperventilation causes decreased CO2 and compansated respiratory alkalosis NWAC Hormonal influences
TILT 27º angle - Left side - Human wedge compression of the aorta by the gravid uterus causes 30% of cardiac output sequestered chest compressions need to be stronger due to the increased breast size and chest wall resistance intubation is difficult due to the pharyngeal and nasal oedema NWAC Pregnant CPR
Danger: safety for self, others and woman Response: level of consciousness Airway: open the airway Breathing: 2 initial breaths provide positive-pressure ventilations Circulation:30 chest compressions to 2 breaths Defibrillation: assess and shock VF or pulseless VT NWAC CPR
Airway Ensure airway is patent and protected from aspiration Consider early intubation Breathing Confirm placement of tube Secure device Confirm adequate oxygenation NWAC CPR
Circulation Establish IV access Identify rhythm and monitor Administer appropriate drugs Differential diagnosis Search for identified reversible causes NWAC CPR
Adrenaline 1 mg IV bolus repeat every 3-5 min Be aware of all the drugs are on the emergency trolley NWAC Drugs for resuscitation
4 minute after arrest Maternal apnoea occurs associated with rapid declines in arterial pH and PO2 Fetus of an apnoeic and asystolic mother has ≤2 minutes of oxygen reserve After 4 minutes without restoration of circulation, dramatic action must occur NWAC 4 minute rule
The arrest must be witnessed Skilled personnel and equipment available No spontaneous maternal circulation for 4 min Potential viability: singleton at 23-24 weeks or greater A perimortem caserean section can save two lives NWAC Pre-requisite for perimortem caserean
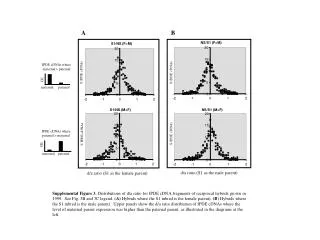
Occurs when there is an opening between the amniotic sac and the uterine veins in approximately 1:20 000 births Risk factors include Abruption Intrauterine fetal demise Tumultuous labor Oxytocin hyperstimulation NWAC Amniotic fluid embolism (AFE)
Amniotic fluid may enter maternal circulation passes through the maternal heart and becomes trapped in maternal pulmonary circulation causing L sided heart failure and bronchospasm These lead to localised DIC which then spreads quickly throughout the mother Anaphylactic reaction associated with amniotic fluid in the maternal circulation may occur NWAC AFE
Symptoms occur very rapidly Sudden dyspnoea and respiratory distress Shock without obvious blood loss Maternal collapse Seizures (30%) DIC Diagnosis is usually made postmortem NWAC AFE
Call for help Supportive and resuscitative ABC 2 large bore cannulae Consider X-ray and ECG Immediate delivery NWAC Management
Rare obstetric emergency with very poor prognosis for maternal-fetal outcome Historically high maternal mortality rate of 85% declined to 27% with better diagnosis and ICU treatment NWAC Summary of AFE
Cardiac arrest is a rare event 44-50% of maternal deaths are preventable by improving management strategies Remember 27ºº tilt and working around the increased breast tissue Perimortem C/S can save 2 lives TEAM WORK can help to improve outcomes Documentation and Debriefing are of utmost importance NWAC CONCLUSION
NWAC Scenario • 38 year-old parturient at 34 weeks’ gestation suffering from dyspnea and chest pain is admitted to the ER • Vital signs • AConscious • BSianosis, RR 40 breath min-1, SpO2 85%during 15 L/min oxygen via reservuar mask • CHR140 beat min-1 sinus tachycardia, BP 70/40 mmHg • D Anxiousand restless • EGravid uterus • Differential diagnosis?
NWAC Scenario continued All of a sudden she became unconscious and apnoeic ECG monitor displays wide complexes, HR 20 beat min-1. No pulse What do you do right now?