Download
1 / 82
820 likes | 877 Views
Dive into the complexities of human inheritance patterns with a focus on Mendelian laws, pedigree analysis, and genetic disorders. Learn about autosomal dominant traits and the characteristics of specific genetic diseases.

E N D
Mendelism, Patterns of Human InheritanceBy: MahdiBijanzadeh MD, PhD.bijanzadeh-m@ajums.ac.ir
Mendelism,Patterns of Human Inheritance At the end of this session, you should: Analyse and evaluate different pedigrees and answer these questions: 1. What are specialties of α –Thalassemia? 2. What are specialties of Hemophilia A? 3. What is difference between X syntery diseases and X-linked diseases?
Human genes: 1. Nuclear: Autosome X-linked Y-linked 2. Mitochondrial (Cytoplasmic) OMIM ( Online Mendelian Inheritance in Men): 3917 Mendelian diseases: 84% due to mutation in 1990 genes (8% genome) 16% due to mutation in unknown genes. >16,000 traits or disorders exhibit single gene unifactorial or Mendelian inheritance. 2% general population: generally in childhood, 10% after puberty & 1% after fertility. Patterns of Human single gene Inheritance
Terminology • Locus • Allele (Allelomorph): Wild-type Mutant • Haplotype • Mutation • Variants • Polymorphism • Genotype • Phenotype
Terminology • Single gene disorders: • Homozygous (homozygote) • Heterozygous (heterozygote) • Compound heterozygote • Hemizygous • Mitochondrial DNA • Sex influenced • Sex limited
Pedigree • Kindred • Proband, (propositus/ proposita), index case • Consultand • Sibs: sibship • First degree • Second degree • Third degree: first cousins • Forth degree: Second cousin • First cousin once removed
Pedigree • Isolated case • Sporadic case • Fitness • Important affects: penetrance: % • expressivity: variable
Mendelian heredity The Mendelian laws of inheritance: • The law of independent assortment. Specific traits operate independently of one another. • The law of independent segregation. Inherited characteristics exist in alternative forms, today known as alleles. For each characteristic, an individual possesses two paired alleles. • The law of dominance. For each characteristic, one factor is dominant and appears more often, in a definite 3:1 ratio. The alternative form is recessive. This constant ratio represents the random combination of alleles during reproduction.
Mendelian heredity • Heredity pattern depends to: • 1. Phenotype: dominant : pure or complete D. • incompletely D. (SemiD.) • codominant • recessive: (loss of function: 50%) • 2. Chromos. location: autosome • (sex influenced, sex limited) • sex: X syntery, Y syntery • X-linked, Y-linked • Pseudoautosomal
Autosomal Dominant - High incidence in geographical areas & big list of them. - Transferred in families, MR. or SR. → Social problems - Disease phenotype seen in all generations. - Normal parents no transmit to children, child risk: 50% - Equal chance for male and female - D/D is rare due to fitness=0 • New mutation possible • Sometimes called 'vertical' transmission and is confirmed when male-male transmission is observed.
Autosomal Dominant • Peliotropy: single gene that may to 2 or more apparently unrelated effects: tuberous sclerosis: a range of: learning difficulties, epilepsy, a facial rash known as adenoma sebaceum (composed of blood vessels and fibrous tissue known as angiokeratoma) or subungual fibromas. • Sometimes an individual with a mutation is entirely normal. • Variable expressivity: PCK, NF1. • Reduced penetrance or skipping a generation, may be due to modifying effects of other genes, as well as interaction of gene with environmental factors.
New Mutation: Achondroplasia. • Co-Dominance: 2 allelic traits that both expressed in heterozygous state: AB blood group. • Homozygosity for AD traits: affected individuals more severely affected (achondroplasia) or have earlier onset age (familial hypercholesterolemia) or not more severely affected (Huntington & myotonic dystrophy).
Autosomal Dominant Neurofibromatosis I (NF 1): NF 1 • 1 in 3500 live birth, the most common AD. • Neurofibromas, café au lait spot, Lisch nodules (iris hamartomes) and less common: MR, CNS tumors &… • Mutations in Neurofibromin gene→ loss of function, ½ new: in consult should be detected is that sporadic or from parents (different risk for sibs no for offspring). • Penetrance: 100% in adults, with variable expressivity
Familial hypercholestrolemia: incomplete, homozygote is more severe than heterozygote. Mutation in LDLR gene → increase plasma & ↓hepatic clearance of LDL →atherosclerosis & thrombosis → MI & ischemia Hypercholestrolemia from first decade. Arcus corneas, tendon xanthomas, polyarthritis, CAD. Untreated: 100% risk (75% females) for CAD development by age of 70years. Autosomal Dominant
Autosomal Dominant Achondroplasia: incomplete • The most common cause of human dwarfism, mutation in FGFR3 → shortening of long bones & abnormal differentiation of other bones. • Shortening of arms & legs, relatively long & narrow trunk, lordosis, macrocephaly, midface hypoplasia & prominent forehead, dental crowding →obesity, lumbar spinal stenosis, central apnea →(10%) die in first year of life. Generally with normal IQ. • Radiographic & sonographic PND available. • New mutation: sudden unexpected appearance of a condition as a result of a mistake in gene transmission.
Autosomal Dominant • Familial testoxicosis: • sex-limited: expressed in only one sex. • Mutation in Luteinizing hormone (LCGR) coding gene→ activates receptor signaling even in absence of the hormone • Develop secondary sexual characteristics & adolescent growth spurt at 4 years. • Normal fertility
Autosomal Dominant • Marfan Syndrome (MFS), congenital contractual arachnodactyly • Disorder of fibrous connective tissue. • FBN1 gene on 15q21. • Patients are tall compared with unaffected family members, have joint laxity, a span: height ratio greater than 1.05, a reduced upper to lower segment body ratio, pectus deformity, and scoliosis.
Autosomal Dominant • Diagnosis: where family history is non-contributory, is made when patient has a minimum of 2 major criteria + involvement of a third organ; for a person with a close relative who is definitely affected, it is sufficient to have one major criterion + involvement of a second organ system.
Autosomal Dominant • Hantington disease: complete AD, HD, progressive neurodegenerative disorder..
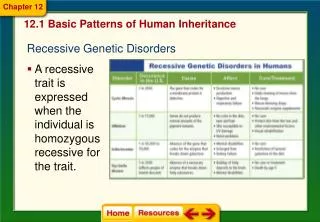
Autosomal Recessive • Only in homozygotes or compound heterozygotes • One normal gene can inhibit mutant allele. • Generally due to loss of function mutations: 50% function • Proband generally is alone, or along with sibs. • Equal chance for male and female. • Patient’s parents are carriers of mutant alleles. • Risk for any of sibs: ¼ • Rare new mutation
Autosomal Recessive Consanguinity: increase risk of two parents mutation. Mutant alleles are generally in carriers transferred during generations without disease. Definition: Consanguinity is a strong evidence, but not prooffor rare AR. Risk is 2-3% for non-consanguinity & 3-5% for consanguinity. The most common explanation is sporadic & non-consanguinity. The rarer, the most consanguinity: Xeroderma pigmentosum, Tay-sachs disease
Autosomal Recessive • Heterozygous show no features of disorder and are perfectly healthy; they are described as carriers. • No possible to trace trait or disorder through family, as all affected individuals in a family are usually sibship. • Pseudodominance: a homozygous and a carrier of same disorder, their offspring have a 1 in 2 (50%) chance.
Autosomal Recessive Locus Heterogeneity: A disorder inherited in same manner can be due to mutations in more than one gene. • by virtue of their involvement in community, if two affected persons were homozygous for same recessive gene, all of their children would be similarly affected. Families have been described in which all children born were perfectly normal, because parents were homozygous for mutant alleles at different loci.
Autosomal Recessive • Sensorineural hearing impairment/deafness: 30 genes and a further 50 loci have been shown. • Retinitis pigmentosa. • Autosomal recessive microcephaly. • Genocopy: disorders with same phenotype from different genetic loci. • Phenocopy: same phenotypes results from environmental agents.
Autosomal Recessive • Allelic heterogeneity or mutational heterogeneity: In majority of single-gene disorders a large number of different mutations have been identified as responsible: thalassemia, CFTR. • Most individuals with an AR. disorder are probably compound heterozygotes rather than true homozygotes, unless their parents are related, when they are likely to be homozygous for same mutation by descent, having inherited same mutation from a common ancestor.
Autosomal Recessive • Thalassemia: α , β • Cystic fibrosis • Xeroderma pigmentosa Exception: Sex-influenced: • (Familial) Hemochromatosis
Autosomal Recessive Thalassemia (α or β): > 200 mutations, del. of α-globin gene: ↑80% of α-thalassemia ~ 15 mutations: ↑90% of β-thalassemia Deficient synthesis of α or β-globin→ • Inadequate Hb production→Hypochromia microcytosis anemia • Unbalanced globin→ ineffective Erythropoisis & hemolytic anemia Prenatal diagnosis is possible (amniocentesis or CVS)
β-thalassemia trait: an allele mutation: usually asymptomatic, mild hypochrome microcytosis anemia, mild BM erythroid hyperplasia & occasionally hepatosplenomegaly. • β-thalassemia major: severe hypochrome microcytosis anemia, growth retardation, jaundice, hepatosplenomegaly (extramedullary hemotopoisis) , BM expansion & short lifetime.
Autosomal Recessive Cystic Fibrosis (CF): 1/313-1/90,000 • Inheritance risk: couples with CF → prenatal diagnosis. • Mutation in CF transmembrane conductance regulator gene (CFTR) → disorder of epithelial ion transport, Cl, Na in respiratory, pancreas, biliary system, intestine, sweat glands and male genitalia. • Dehydrated secretions in lungs → rec. infections → respiratory failure. • Pancreas fibrosis/ increased sweat NaCl (Salty baby syn.) • Poor growth and meconium ileus in children, • Azoospermia: 95%
Autosomal Recessive Xeroderma pigmentosa: consanguinity: inbreeding • Reduced or absence capacity for global genome repair → oncogenic mutations, highly UV specific. • 1-2 years old: sunburning, acute photosensitivity, freckling, photophobia, skin aging, premalignant actinic keratosis, benign and malignant neoplasms: BCC, SCC • Ocular abnormality (60-90%), neuropathy (18%) • Internal neoplasms: CNS, leukemia, lung & gastric • Shortened life span. • prenatal diagnosis by functional testing of DNA repair & UV sensitivity
Autosomal Recessive • Familial Hemochromatosis: • sex-influenced: F:1/5-1/10M Mutation in HFE gene: (Cys282Tyr): increase ferrous absorption → storage in heart, liver & pancreas. • Due to less absorption, less alcoholism & more loss. • Fatigue, arthralgia, arthritis, ↓libido, abdominal pain, hepatomegaly, cirrhosis, DM, cardiomyopathy, hepatocellular carcinoma, … • Elevated Transferin iron or Ferritin.
X-linked heredity • X contains 1100 genes (Y contains 86 genes). • Male: X → 2genotypes: hemizygous allele • Female: 2X → 3genotypes: Female: X inactivation: gene expression is same in M/F. Percentile of mutant alleles on active X → phenotypes, so believed that X-linked is a spectrum, not R. or D.
X-linked Recessive • Phenotype expressed in all male carriers and only in homozygote female. • Diseases limited to male and rare in female. • Gene passes from father to all daughters, no sons. • Diseases transmitted by healthy heterozygous female carriers to affected males, and by affected males to their obligate carrier daughters (50% risk for sons), with a consequent risk to male grandchildren through these daughters: Knight move. • Male with a mutant allele on his single X chromosome is hemizygous for that allele.
X-linked Recessive • Female carrier →manifesting heterozygote due to unbalanced or skewed inactivation. • Hemophilia A (Royal Hemophilia) • Gene present in both parents →homozygote patient daughter, rare but in consanguinity: Color blindness • Hemophilia B • Duchenne muscular dystrophy (DMD) • Wiskott-Aldrich syndrome
Hemophilia A (Royal Hemophilia): Samein all ethnics: 1/5000-10000 male neonates Mutation in F8 →deficiency or dysfunction of clotting factor VIII: agglutination problems Classically a male disease, although rarely female due to skewed X inactivation. Severe : cephalohematomas or umblical bleeding/ Moderate: begin to walk/ Mild: hemarthroses or bleeding after trauma Treatment: Factor replacement/ Liver transplantation X-linked Recessive