Download
1 / 29
290 likes | 536 Views
Prof. Bettina Borisch, FRCPath Institut de médecine sociale et préventive Département de pathologie et immunologie Hôpitaux universitaires de Genève Université de Genève bettina.borisch@medecine.unige.ch. Squamous cell carcinoma in the oral cavity and cervix.

E N D
Prof. Bettina Borisch, FRCPath Institut de médecine sociale et préventive Département de pathologie et immunologie Hôpitaux universitaires de Genève Université de Genève bettina.borisch@medecine.unige.ch Squamous cell carcinoma in the oral cavity and cervix Zürich-5-nov-2008
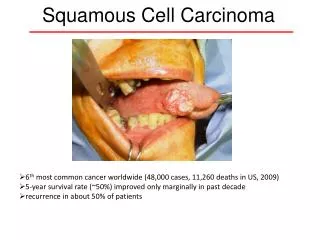
Zürich-5-nov-2008 Carcinoma of the uterine cervix and oral squamous cell carcinoma? What do they have in common? • Carcinoma of the uterine cervix is the second most common female malignancy in the world • Oral squamous cell carcinoma is a major cause of cancer morbidity and mortality worldwide
Zürich-5-nov-2008 Carcinoma of the uterine cervix and oral squamous cell carcinoma? What do they have in common ? • Cervical cancer is a world wide disease but early detection has reduced the mortality in affluent countries. • Oral cancer has the highest incidence in developing countries, especially among tobacco and alcohol users and betel quid chewers.
Zürich-5-nov-2008 Estimated numbers of incidence and mortality of cancers in women worldwide in 2002(Data shown in thousands)
Zürich-5-nov-2008 Estimated numbers of incidence and mortality of cancers in men worldwide in 2002(Data shown in thousands)
Zürich-5-nov-2008 Male and female cancers worldwide in 2002
Zürich-5-nov-2008 Carcinoma of the uterine cervix and oral squamous cell carcinoma? What do they have in common ? • They both derive from epithelia that are similar , upper aero digestive tract mucosa and that of ectocervix and vagina • non keratinizing squamous epithelia • Epithelia that undergo stepwise maturation from immature basal layer cells to surface keratinocytes • Strong association of cervical and oral cancer with human papillomavirus (HPV)
Zürich-5-nov-2008 Human papillomavirus (HPV) • HPVs are epitheliotropic DNA viruses present in the skin and mucosa • More than 70 types have been described • Mucosal and genital HPVs are divided into low risk (HPVs 6,11,42,43,44) and high risk (HPVs 16,18,31,33,35,45,51,52,56) • High risk HPV infection contributes to carcinogenesis and tumor progression through two viral oncogenes: E6 and E7
Zürich-5-nov-2008 Two viral oncogenic proteins • E6 and E7 oncogenes encode proteins of about 151 and 98 amino acids, respectively • E6 forms a complex with p53, loss of p53 leads to deregulation of the cell cycle • E6 prevents senescence by upregulation of telomerase • E7 forms complexes with RB family proteins, negative regulators of cell growth, releases E2F, that induces cell cycle progression via host genes (upregulation of Cyclin E and p16INK4) • E6 and 7 are critical in extending the life span of epithelial cells – a necessary component of tumour development
Zürich-5-nov-2008 Molecular evidence linking HPV to cancer in general and to cervical cancer in particular • HPV-DNA is detected by hybridisation techniques in over 95% of cervical cancers • Specific HPV types are associated with cervical cancer (high risk) versus condylomata (low risk) • Viral genes disrupt cell cycle (E6 and E7) • However, the evidence does not implicate HPV as the only factor
Zürich-5-nov-2008 Risk factors for cervical cancerMolecular - epidemiologic data • Early age at first intercourse • Multiple sexual partners • Increased parity • A male partner with multiple partners • The presence of cancer-associated HPV • Persistent detection of high-risk HPV • Exposure to oral contraceptives and nicotine • Genital infections (chlamydia)
Zürich-5-nov-2008 Approximate lifeftime risks In percentage of the whole population • Exposure to HPV 75% • Exposure to high risk HPV 50% • Persistent high grade CIN 10% • Invasive carcinoma 1.3% • Dying of cervical cancer 0.4%
Zürich-5-nov-2008 Human papillomavirus (HPV) • HPV is an obligatory intranuclear organism that must infect mitotically active cells in order to establish infection in the epithelium • Infection has to access the basal cells of multilayered epithelium in 3 different ways: • Mucosal injury, metaplastic epithelium or squamo-columnar junction
Zürich-5-nov-2008 Fate of epithelial HPV-infection Mitotically active cell reached by HPV: • 1) latent infection, viral replication is connected with the cell cycle, cells appear morphologically intact • 2) latent infection may convert into replicative infection, in terminally differentiated cells the complete virion assembles • 3) The majority of initial infections become virus-free spontaneously
Zürich-5-nov-2008 Histology of CIN I H&E HPV - ISH Ki 67 p16INK4
Zürich-5-nov-2008 Link cervical cancer – HPV well established • What is the evidence linking HPV infection with cancers of the oral cavity including head and neck? • Oral/Head and neck squamous cell carcinoma (O/HNSCC) is a locally aggressive disease. Some areas traditionally report a high incidence (France, South India, Eastern Europe, Japan). Tobacco and alcohol are well established risk factors
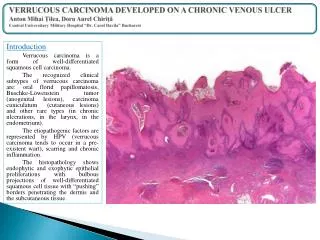
Zürich-5-nov-2008 Viral replication in oral epithelia • Koilocytes, atypia, akanthosis, epithelial thickening • Basal layers of squamous cell epithelium of the oral cavity or oropharynx • At the reserve cell layer in the respiratory epithelium • In the larynx, metaplastic alteration, multilayered squamous cell epithelium, papillomas and finally carcinomas develop
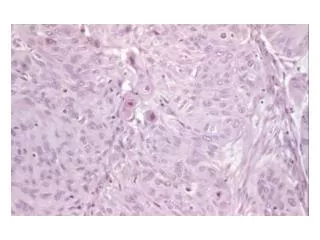
Zürich-5-nov-2008 Moderately diff Well differentiated Poorly differentiated Oral/HN Squamous cell carcinoma Basaloid SCC Verrucous carcinoma Other variants: Spindle Papilllary Adenosquamous acantholytic
Zürich-5-nov-2008 Detection of HPV in OHNSCC / HPV-prevalence in OHNSCC • The results vary and depend on the detection method used (usually HPV general primer sets) • Initial studies in the 80ies • The reported overall frequency of HPV DNA in OHNSCC varies from 14-61%, (46.5%) • Multiple infections are relatively common (22-48%) • Close association between infection and a subset of OHNSCC with basaloid / verrucous histological features
Zürich-5-nov-2008 Correlation presence of HPV and histological features Szentirmay et al. 2005
Zürich-5-nov-2008 HPV phylogeny and oral cancer • All « genital or mucosal » types of HPV belong to supergroup A • Within supergroup A eleven subgroups have been defined on the basis of genetical and biological similarities • Groupe A2 are mainly in skin warts, A 6,7 and 9 in genital high grade dysplasia and carcinoma • A 6,7,9,10, and 11 are the most frequently occuring types in the head and neck region
Zürich-5-nov-2008 Phylogram of human papillomaviruses (HPVs) belongingto supergroup A. The sequence name is displayed at the end of eachline. The values on the graph show the distances of evolution.
Zürich-5-nov-2008 Modes of transmission • It is generally accepted that transmission of genital infections is associated with sexual contacts • What about the head and neck region ? • Perinatal transmission to neonates at birth has been described • Some HPV types in newborns have not been found in their mothers • Oral-genital or oral-anal sex • Multiple pathways for HPV transmission
Zürich-5-nov-2008 Natural history of HPV infection in the oral / HN region • The general presence of HPV in normal oral mucosa has not been defined yet • Sampling of healthy cells is not standardized (basal cell layer) • 1-60% positivity, (probably 10%) • HPV may colonize healthy mucosa, which later leads to malignant transformation
Zürich-5-nov-2008 Kaplan – Meier curves of 114 cases of oral or laryngeal carcinomas HPV as an prognostic factor in oral / HNSCC?
Zürich-5-nov-2008 HPV16 in oral squamous cell carcinoma:Clinical correlates and 5-year survival Sugiyama et al. 2007, Br J Oral Maxillofacial Surg
Zürich-5-nov-2008 Clinicopathological correlates • Patient with HPV+ oral cancers are young, non-drinkers, non-smokers, female • Prognostic significance of HPV is still under debate • Recent data suggest that NFkB family proteins such as p65 in HPV infected oral cancer may be linked to improved differentiation and better prognosis of the disease when treated • Molecular biology: frequent LOH 3p and 9p21, inactivation of p16 gene, LOH at 17p with mutation of the p53 associated with progression
Zürich-5-nov-2008 Open questions : • Why HPV is found in virtually all cervical cancers, but only a subset of oral carcinoma has yet to be explained • HPV is rarely found in premalignant oral lesions, and may therefore not be necessary for the progression of oral mucosa to malignancy • HPV detection for patient management on the oral setting? • Simple screening test such as exfoliative cytology in oral mucosa lesions - feasable ? • More insights into pathogentic factor interplay • Vaccin for HNSCC?