Download
1 / 31
330 likes | 463 Views
Explore how psychological factors contribute to athletic injuries, stress-injury relationships, emotional reactions, and the role of sport psychology in rehabilitation.

E N D
chapter 19 Athletic Injuries and Psychology
Session Outline • Psychological Factors in Athletic Injuries • How Injuries Happen—Psychological Antecedents • Explaining the Stress–Injury Relationship • Typical Psychological Reactions to Exercise and Athletic Injuries • Role of Sport Psychology in Injury Rehabilitation
Psychological Factorsin Athletic Injuries • Some 3 to 17 million people are injured each year in sport and exercise. • Physical factors are the primary causes of injury, but psychological factors can also contribute.
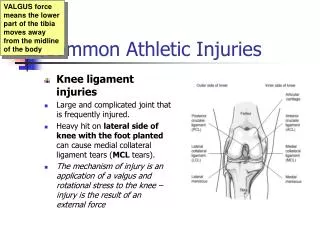
How Injuries HappenPsychological Antecedents Personality factors To date, personality factors associated with athletes’ injuries have not been successfully identified. Stress levels People with high levels of life stress have more sport- and exercise-related injuries.
Stress–Athletic Injury Model Adapted, by permission, from J. Williams and M. Anderson, 1988, "A model of stress and athletic injury: Prediction and prevention," Journal of Sport and Exercise Psychology 10(3): 297.
How Injuries HappenPsychological Antecedents The stress–injury relationship is complex. • Smith and colleagues (1990) found that life stress related to injuries only in “at-risk” athletes (those with few coping skills and low social support). • Individuals who have low self-esteem, are pessimistic and low in hardiness, or have higher levels of trait anxiety experience more injuries or loss of time due to injuries. (continued)
How Injuries HappenPsychological Antecedents (continued) The stress–injury relationship is complex. • The greatest stress sources for injured athletes were not the physical aspects but the psychological ones (e.g., fear of reinjury, shattered hopes or dreams). • Teaching stress management can reduce risk of injury and illness.
Explaining the Stress–Injury Relationship Attentional disruption Stress disrupts an athlete’s attention by reducing peripheral attention and causing distraction and task-irrelevant thoughts. Increased muscle tension High stress can cause muscle tension and coordination interference.
Explaining the Stress–Injury Relationship Other stress–injury relationship explanations: • Overemphasis on acting tough and a “giving 110%” attitude • Failure to distinguish between normal discomfort and injury pain • “You’re injured, you’re worthless” attitude
Physiologic Components of Athletic Injury Stress • Psychological stress increases catecholamines and glucocorticoids, which impair the movement of healing immune cells to the site of the injury and interfere with the removal of damaged tissue. • Prolonged stress may also decrease the actions of insulin-like growth hormones that are critical during the rebuilding process. • Stress also causes sleep disturbance, another factor identified in interfering with physiologic recovery.
Psychological Reactions to Exercise and Athletic Injuries Three general categories of emotional reactions to being injured: • Injury-relevant information processing • Emotional upheaval and reactive behaviors • Positive outlook, coping
Psychological Reactions to Exercise and Athletic Injuries Keys Most people experience a typical response to injury, but the speed and ease with which they progress through stages can vary widely. The period immediately following injury is characterized by the greatest negative emotional reactions.
Other Injury Reactions Identity loss When athletes can no longer participate because of an injury, they may experience a loss of personal identity. That is, an important part of themselves is lost, seriously affecting self-concept.
Other Injury Reactions Fear and anxiety When injured, athletes can experience high levels of fear and anxiety. They worry whether they will recover, if reinjury will occur, and whether someone will replace them permanently in the lineup. Because the athletes cannot practice and compete, there’s plenty of time for worry.
Other Injury Reactions Lack of confidence Given the inability to practice and compete and their deteriorated physical status, athletes can lose confidence after an injury. Lowered confidence can result in decreased motivation, inferior performance, or additional injury because the athletes overcompensate.
Other Injury Reactions Performance decrements Because of the lowered confidence and missed practice time, athletes may experience postinjury performance declines. Many athletes who have difficulty lowering expectations after an injury expect to immediately return to a preinjury level of performance.
Signs of Poor Adjustmentto Athletic Injuries • Feelings of anger and confusion • Obsession with the question of when one can return to play • Denial (e.g., “The injury is no big deal”) • Repeatedly coming back too soon and experiencing reinjury • Exaggerated bragging about accomplishments (continued)
Signs of Poor Adjustmentto Athletic Injuries (continued) • Dwelling on minor physical complaints • Guilt about letting the team down • Withdrawal from significant others • Rapid mood swings • Statements indicating that no matter what is done, recovery will not occur
Poor Adjustment to Injury: Getting Professional Help When abnormal emotional reactions to injuries are identified, a referral to a sport psychologist or another qualified mental health provider should be made just as should be the case if an uninjured athlete exhibits general life problems (e.g., depression, severe generalized anxiety) of a clinical nature.
Roles of Sport Psychologyin Injury Rehabilitation Keys • A holistic approach is needed, emphasizing the healing of both the mind and body. • Psychological factors play an important role in injury recovery (Ievleva & Orlick, 1991). • Injury treatment should include psychological techniques to enhance the healing and recovery process. • Athletes will not automatically transfer psychological skills used in athletics (e.g., imagery) to the injury rehabilitation situation. (continued)
Roles of Sport Psychologyin Injury Rehabilitation (continued) Keys Using relaxation and imagery during rehabilitation reduces anxiety and was associated with greater knee strength in athletes after knee surgery. Psychological factors (e.g., self-talk, goal setting, self-motivation) also positively affect adherence to injury treatment protocols.
Role of Sport Psychologyin Injury Rehabilitation Understand the three-phase process of rehabilitation and recovery: 1. Injury or illness phase 2. Rehabilitation and recovery phase 3. Return to full activity phase
Role of Sport Psychologyin Injury Rehabilitation Each phase dictates different approaches to the psychology of recovery. • Injury or illness phase—focus on helping the athlete understand the injury. • Rehabilitation or recovery phase—focus attention on helping sustain motivation and adherence to rehabilitation protocols through goal setting and maintaining a positive attitude. (continued)
Role of Sport Psychologyin Injury Rehabilitation (continued) Each phase dictates different approaches to the psychology of recovery. • Return to full activity phase—although an athlete is physically cleared for participation, complete recovery does not happen until normal competitive functioning occurs.
Role of Sport Psychologyin Injury Rehabilitation • Build rapport with the injured party: Take the athlete’s perspective, provide emotional support, and be realistic but positive and optimistic. • Educate the injured person about the injury and recovery process. (continued)
Role of Sport Psychologyin Injury Rehabilitation (continued) • Teach specific coping skills: Discuss goal setting, positive self-talk, imagery, visualization, and relaxation training. • Teach how to cope with setbacks. • Foster social support. • Learn from injured athletes. (continued)
Role of Sport Psychologyin Injury Rehabilitation Guidelines for providing social support • Provide social support to athletes (sources of support include coaches, significant others, and medical personnel). • Athletes generally turn to coaches and medical professionals for informational support and to family and friends for social support. • Social support needs to vary across rehabilitation phases.
Role of Sport Psychologyin Injury Rehabilitation • The need for social support is greatest when setbacks occur or when other life demands place additional stress on athletes. • While generally helpful, social support can have negative side effects (e.g., when the support provider does not have a good relationship or have credibility with the athlete or when support is forced).
Recommendations for Coping With Injuries for Other Injured Athletes • Accept and positively deal with the situation. • Focus on quality training. • Set goals.
Recommendations for Facilitating Rehabilitation for Coaches • Foster coach–athlete contact and involvement. • Demonstrate positive empathy and support. • Don’t repeatedly mention injury in training.
Recommendationsfor Facilitating Rehabilitationfor Sports Medicine Personnel • Educate and inform athletes about injury and rehabilitation. • Foster positive interaction and customize training. • Demonstrate competence and confidence.