Download
1 / 39
400 likes | 516 Views
Learn about the loop of sensory, cognitive, and behavioral functions in cognitive rehabilitation, identifying areas of impairment, compensating mechanisms, and challenges faced for brain restoration. Dive into brain functions like brain stem, diencephalon, sensory functions, and executive functions for effective retraining. Discover evidence-based cognitive rehabilitation strategies and a case study following extensive cognitive rehabilitation.

E N D
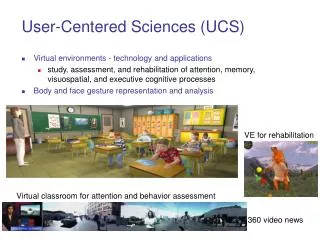
Computerized Cognitive Rehabilitation—Evidence and case study demonstration Michael Gilewski, PhD Neuropsychologist Dept. of Physical Medicine & Rehabilitation LLU School of Medicine
Learning Objectives • To verbalize the loop of sensory, cognitive and and behavioral functions that cognitive rehabilitation or any learning needs to utilize • To state which cognitive functions demonstrate the greatest evidence for training efficacy • To understand areas of benefit achieved by subject with severe brain injury in case study following extensive cognitive rehabilitation
Related issues not addressed • The brain is universal. Although the focus is on application to brain injury, the same principle underlie any learning • Will not address cognitive enhancement in healthy adults • There are many Web-based or local computer programs available. Time won’t allow elaboration on efficacy of each of these • Come to poster for demonstration of the cognitive rehabilitation program in this talk. • Can entertain some questions but feel free to email me for information of details resources and such.
This program has been approved to meet the School of Medicine’s promotion criteria for CME for Education.
Computerized cognitive rehabilitation: Brain REHAB basics
What is Cognitive Rehabilitation? • A brain injury often dismantles the capacity for or at least timing and coordination of various brain functions Antonio Damasio – “In the brain, timing is everything!” • Cognitive rehabilitation follows a process of: • Identifying areas of impairment • Facilitating compensatory mechanisms to rapidly improve some function • Challenging the brain to restore function
Retrain the brain from the bottom up • Brain stem: wakefulness, internal self-regulation, attentional control, basic sensory coordination • Compensation: Routine and daily structure, managing energy, checking in with oneself, balanced rest and activity • Goldilocks as role model • Challenge: Constant striving for balance, improve internal awareness, mindfulness, meditation, and increased focused, sustained and challenged attention • Physical balance is very important; also basic coordination of eyes, vestibular system and body in motion
Retrain the brain from the bottom up • Diencephalon: Thalamus, hypothalamus and radiating pathways for basic brain activation • Control of stimulation, sleep, hormonal control and regulation of complex internal states, emotional control • Compensation: Breathing and other relaxation, daily schedule, external control of drives, adapt environment to needs, “retreat,” accept feedback from others, general stress management • Challenge: Gradual building of stimulation tolerance, controlled increase of behavioral control, shift from supervision to self-control, learn from mistakes, discover chain of acceleration to problems
Retrain the brain from the bottom up • Sensory functions: Accurate perception of somatosensory, auditory and visual stimuli as it builds from simple to complex • Compensation: Simplify input, increase ease of perception, use external feedback to check for accuracy • Challenge: Gradual building of accuracy and speed with simple stimuli to more complex integration of information, activate both hemispheres, complex aspects of nonverbal and verbal communication, complex nonverbal visual discrimination and written material, academic and intellectual capabilities, and integration with memory • The focus of much of cognitive rehabilitation
Retrain the brain – then top down • Executive functions: Directing attention, motor control, thinking, complex language, behavioral activation and control • Compensation: SLOW DOWN, stop and think, accept and learn from feedback on errors • Challenge: Maintain goal focus despite distraction, divide attention, activate and shift set with task demands, complex thinking (abstract, divergent thinking, inductive and deductive reasoning…), monitor and predict performance • Another major area of focus in cognitive rehabilitation
Retrain the brain – then top down • Cerebellum: “Software library” of skills and habits, judgment, timing and coordination of thinking/action with situation • Compensation: errorless learning, frequent small practice, evidence of results, build behavior chains, use routines to compensate for effortful thinking problems • Challenge: Increase speed while maintaining accuracy, go up skill difficulty ladder, learn a new skill
Cognitive Rehabilitation: Evidence • Source: Keith Cicerone et al., Arch Phys Med Rehabil, 2000, 2005, 2011 • Beta version of evidence-based Cognitive Rehabilitation Manual (Edmund Haskins, 2011) through American Congress of Rehabilitation Medicine www.acrm.org
Cognitive Rehabilitation: Evidence • Attention • Practice standard for remediation of attention after brain injury • Practice option for computerized attention training with therapist involvement and intervention • Visual-spatial/praxic functions (selected) • Practice standards for remediation of left neglect in right brain stroke and gestural strategies for apraxia with left brain stroke • Practice options for systematic training of visuospatial deficits and visual organization skills and for computerized training to expand visual fields
Cognitive Rehabilitation: Evidence • Language/communication • Practice standard for language skill training in left brain stroke and social communication deficits in traumatic brain injury • Practice guidelines for language formulation and reading and for greater treatment intensity with left brain stroke • Practice options for group or computerized interventions for cognitive linguistic deficits • Memory • Practice standard for memory strategy training with mild TBI • Practice guideline for external compensation strategy training for severe deficits • Practice options for errorless learning techniques and group interventions
Cognitive Rehabilitation: Evidence • Executive functions • Practice standard for metacognitive strategy training (self-monitoring and self-regulation) • Practice guideline for training in formal problem solving strategies related to functional problems and everyday situations • Practice options for group-based interventions of executive deficits and problem solving
Subject DN • Man who suffered a severe anoxic brain injury following several episodes of ventricular cardiac arrest in June 2008 • After internal defibrillator and medical stability, went through a course of acute inpatient rehabilitation, intensive outpatient and residential treatment through March 2009. • Discharge to home with full-time caregivers for supervision • May 2010 – wife consulted USC Neurology for other treatment or research • Background • Age 60 at baseline assessment • 14 years education, owned successful film production business • Lives with wife and their daughter (in her 20s)
Anoxic brain injury • Absence of oxygen leads to cell death • Secondary chemical cascade harming or destroying other cells • Typically the poorest prognosis for an acquired brain injury compared to trauma of similar severity, bleeds, nonmalignant tumors, etc. • Anoxia disproportionately affects memory and basic executive functioning • The most vulnerable are watershed areas of brain (depend on distal circulation from two artery systems) or areas of high metabolism (e.g., areas involved in memory consolidation) • Imaging (as for DN) typically reveals widespread atrophy (his was mild to moderate)
A-B-A-B Single Case Study Design • Study aim: Would regular student-assisted computerized cognitive rehabilitation improve cognitive function in this man with a severe anoxic brain injury more than two years post arrest? • June 2010 – Alzheimer’s Coordinating Center neuropsychological test battery at USC • Jun–Dec 2010 - Initial control phase A: OT nonspecific cognitive enhancement with computer 2-3 x/wk • January 2011 – Readminister tests • Feb–Aug 2011 Initial training phase B: Student-assisted computerized cognitive rehabilitation 2-3 x/wk • September 2011 – Readminister tests • Sep–Dec 2011 – 2nd control phase A: Group games and nonspecific cognitive enhancement or computer use 3+ x/wk at residential setting • January 2012 – Readminister tests • February 2012 – started 2nd training phase B
Computerized Cognitive Training • www.neuropsychonline.com • 6 domains, 12 graded tasks/domain, 3-4 difficulty levels per task • Students trained to assist • Attention • Executive functions • Memory • Visuospatial skills • Problem solving • Verbal/nonverbal communication Other cog rehab programs do exist!
NEUROPSYCHOLOGICAL ASSESSMENT • Demographic predicted ability = 86th %ile, AM-NART estimated = 93rd %ile • Blessed and Folstein mental status tests (some items analyzed separately) • Attention – Digit span, Trail Making, Letter-Number Sequencing, Digit-Symbol Coding • Learning-Memory – Logical Memory story, California Verbal Learning Test • Language – Boston Naming, Letter fluency (FAS), Category fluency (animals, vegetables), Token Test (substituted Rule Governed Drawing) • Visual-spatial – Block Design • Geriatric Depression Scale • Added physical – full-tandem standing time and 12-foot walking speed • Added behavior/QOL – Frontal Systems Behavior Scale (FrSBe) and Mayo-Portland Z-scores compared to age norms as possible; change compared to baseline
RESULTS TO DATE Base = raw of total or Z-score ++ Z-score improvement of 1+ + Improve (or – worse) 0.5-1.0 -- Z-score worsening of 1- Mental status – worse but orientation not trained Attention – some sustained improvement in attn capacity and working memory
RESULTS TO DATE Base = raw of total or Z-score ++ Z-score improve of 1+ + Improve (or – worse) 0.5-1.0 -- Z-score worse of 1- Memory is worst cognitive function. Some improvement in recognition.
RESULTS TO DATE Base = raw of total or Z-score ++ Z-score improve of 1+ + Improve (or – worse) 0.5-1.0 -- Z-score worse of 1- Language – Improved naming, generally sustained fluency, some improved Language comprehension. Last assessment performance was very slow.
RESULTS TO DATE Base = raw of total or Z-score ++ Z-score improve of 1+ + Improve (or – worse) 0.5-1.0 -- Z-score worse of 1- Not depressed. Some sustained improvement in brain-related behavior as rated by wife.
Neuropsychonline Cognitive Rehabilitation Therapy System Progress Report - Track 02 - Executive Skills Task 01 - Organizing Information (Commonality)
Track 04 - Visuospatial Skills Progress Report - Task Status
Conclusions • The brain is plastic and can improve even despite severe injury • Computers are one method to facilitate training • Gains will be modest and may sustain • Need lots of practice • Focus training on attention, some executive skills • Include fun/ easy as well as challenge
A recipe for cognitive training • 25% challenge – hard – perhaps 75% correct or worse • 50% enjoyable – modest – 85-90% or better correct • 20% speed – easy but do quickly at 90% or better correct • 5% new learning – pull everything together periodically to learn something new
Thanks Study given a human subjects exemption by USC IRB. • Elizabeth Zelinski, PhD The Rita and Edward Polusky Chair in Education and Aging Professor of Gerontology and Psychology Leonard Davis School of Gerontology, Univ. of Southern California • Teresa Diaz (USC staff) • Student assistants for case study • Natalie Abrahamian • Rachel Anderson • Robert Grijalba • Erin Lee • Joanna Marantidis • Josh Van Zak
Contact Michael Gilewski, PhD LLUHC Neuropsychology East Campus AS-107 909-558-6220 mgilewski@llu.edu