Download
1 / 31
330 likes | 619 Views
Hospital Acquired Catheter-Related Bloodstream Infections (CR-BSI). MED INF 406 - Decision Support Systems and Health Care. Background. More than 5 million Central vascular catheters used annually in US. 250,000 cases of CVC-associated BSIs occur annually in the US

E N D
Hospital Acquired Catheter-Related Bloodstream Infections(CR-BSI) MED INF 406 - Decision Support Systems and Health Care
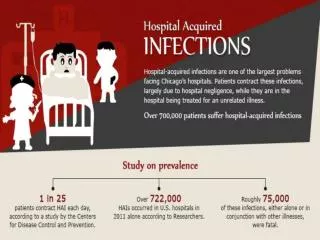
Background More than 5 million Central vascular catheters used annually in US. 250,000 cases of CVC-associated BSIs occur annually in the US ICU related CVC-associated BSIs occuring annually in the US: 80,000 Attributable mortality for these BSIs : upto 28,000 deaths Attributable average cost per infection : $ 56000 Financial Impact! Annual cost of CVC-associated BSIs – upto $2.3 billion • http://www.firstdonoharm.com/HAC/CRBSI/
Definition Bacteremia / fungemia in a patient with an intravascular catheter with: • at least one positive blood culture obtained from a peripheral vein • clinical manifestations of infection (i.e., fever, chills, and/or hypotension) • and no apparent source for the bloodstream infection except the catheter. • Bloodstream infections are considered to be associated with a central line if the line was in use during the 48-hour period before the development of the bloodstream infection. http://www.ihi.org/IHI/Topics/CriticalCare/IntensiveCare/Measures/CatheterRelatedBloodstreamInfectionRate.htm
Impact! • Common in healthcare, especially in ICU • Morbidity (risk for local and systemic infectious complications) • LOS • Mortality • Cost - in term of morbidity and financial resources • As of Oct, 2008 CMS New Rule – No Pay for Never Events Cannot Bill Patient for HAIs http://www.cdc.gov/mmwr/preview/mmwrhtml/rr5110a1.htm
Why Address it ? • 50% of these infections are preventible by the implementation of strategies EvidenceBasedInterventions! This effort should be multidisciplinary: involving • health-care professionals who insert and maintain IV catheters • health-care managers who allocate resources • patients capable of assisting in the care of their catheters
Sources of Infection Skin organisms Environmental contamination Post-placement subcutaneous tract infection Intraluminal contamination Hematogenous seeding
Risk Factors The incidence of CRBSI varies considerably by: • type of catheter • frequency of catheter manipulation • patient-related factors underlying disease acuity of illness
By Catheter pathway from skin to vessel -tunneled -nontunneled • By • Type of Vessel • it occupies • -peripheral venous • -central venous • -arterial CLASSIFYING THE CATHETERS . By Catheter Physical Length - long -short • By the site of insertion • femoral • subclavian • internal jugular • peripheral • peripherally inserted central catheter [PICC • By the intended life span of Catheter • - temp or short-term • -permanent or long-term • or by some special characteristic of the catheter, e.g.: • - presence or absence of a cuff • - impregnation with heparin • antibiotics or antiseptics • and the number of lumens
Risk Factors1. Type of Catheter Peripheral venous catheters • most frequently used devices for vascular access • Low incidence of associated infections BUT Higher frequency of such catheters used SO It adds up! Serious infectious complications produce considerable annual morbidity Central venous catheters (CVCs) • majority of serious catheter-related infections associated with CVCs - especially those that are placed in patients in ICUs
Risk Factors 2. Setting / frequency of catheter manipulation • In the ICU setting, the incidence of infection is often higher: • central venous access needed for extended periods of time • Patient colonization with hospital-acquired organisms • Catheter can be manipulated multiple times per day contamination clinical infection • Catheter insertion in urgent situations with sub-optimal aseptic precautions
Risk Factors 3. Patient Related Factors • Diabetic or high blood glucose levels • Immuno-compromised • Cancer patients • Age - elderly - pediatric population
MultifacetedApproach To improve patient outcome reduce health-care costs strategies should be implemented to reduce the incidence of these infections
The Keystone ICU Project #:Evidence-based recommendations from CDC for preventing CR-BSI • A care bundle of best practices in terms of CRBSIs that individually improve care, but when applied together result in substantially greater improvement. The science supporting the bundle components is sufficiently established to be considered standard of care. (1) Hand Hygiene (2) Full Barrier Precautions during insertion of CVC (3) Cleaning the skin with 2% Chlorhexidine (4) Appropriate site and line selection (5) Remove Unnecessary Catheters # Pronovost P, Needham D, Berenholtz S et al. An Intervention to Decrease Catheter Related Bloodstream Infections in the ICU. N Engl J Med 2006;355:2725-32.
Does patient have peripheral access? • Yes • No • Patient will need one of the following: • Vesicant medication • Vasopressor • TPN • Fuild bolus • Patient needs hemodynamic monitoring • Yes • No • Anticipate IV therapy greater than 5 days • Yes • No
Workflow engine Alert to clinician Central line Alert Populates database with patient names who had the alert associated with them • Patient does not meet criteria: • No peripheral access • IV vesicant • Hemodynamic monitoring • IV therapy greater than 5 days • Decrease the risk of a hospital acquired central line infection by PLACING A PERIPHERAL LINE
Daily Documentation To Justify Keeping A Central Line • High volume IVF • Hi volume blood • Multiple drips • TPN • Limited access • Long term access • Hemodynamic monitoring • Vasopressor/vesicant meds Populates database to track reasons for keeping central lines etc.
Workflow engine Alert to clinician Central line Dwelling Time Alert Dwelling time of central line catheter is greater than 5 days Decrease the risk of a hospital acquired central line infection consider discontinuation of Central line Populates database with patient names who had the alert associated with them
Outcome and Process Measures • Outcome measures • CRBSI/1000 central line days • Average length of central catheter dwelling time • Process measures • Justification of central line • # of alerts rendered and response to them
CDSS Design Guided by the AMIA Roadmap for National Action on CDS vision: “optimal, usable and effective clinical decision support is widely available to providers, patients, and individuals where and when they need it to make health care decisions.”
AMIA RoadMap Pillars • Best Knowledge Available when Needed • High Adoption and Effective Use • Continuous Improvement of Knowledge and CDS Methods
CDSS Framework Service-oriented Architecture (SOA): • An SOA infrastructure allows different applications to exchange data with one another as they participate in business processes. • Core business capabilities are encapsulated within independent software services, and these services are leveraged by various front-end applications to fulfill business requirements.
How did we do ? • Design • Provides a good foundation to build additional CDSS • Reusable, separates knowledge from code • Based on standards • Information availability • Data repository provides robust reporting capabilities • Ability to monitor clinician responses to alert against patient outcomes
What are the Limitations? • Design requires technical resources • Clinician workflow is critical • Be reasonable in expectation of CDSS use
Summary • Information is powerful! Use it to influence clinician practice to positively impact patient outcomes • Performance measures should be monitored to reflect effectiveness • CDSS Design must be re-usable and based on standards • Must lay foundation for additional CDSS
Resources 1. CDC Guidelines http://www.cdc.gov/mmwr/preview/mmwrhtml/rr5110a1.htm 2. Clinical study - An Intervention to Decrease Catheter-Related Bloodstream Infections in the ICU http://content.nejm.org/cgi/reprint/355/26/2725.pdf 3. Clinical study -Prevention of Intravascular Catheter–Related Infections. Leonard A. Mermel, DO, ScM, AM(Hon) http://www.annals.org/cgi/reprint/132/5/391.pdf 4.http://www.journals.uchicago.edu/doi/pdf/10.1086/377265?cookieSet=1 5.A Roadmap for National Action on Clinical Decision Support. Osheroff, MD, Teich, MD, PhD, Middleton, MD, Steen, MA, Wright, Detmer, MD, MA 6. Proposal for Fulfilling Strategic Objectives of the U.S Roadmap for National Action on Decision Support through a Service-oriented Architecture Leveraging HL7 Services – Kawamota, PhD, Lobach, MD, PhD, MS
Bea Dhanoa Marla Husch MariJo Rugh