Head to Toe Assessment
Head to Toe Assessment. https://www.youtube.com/watch?v=cP4zgb9H3Cg Generalized patient assessment Work from the head down Know normal = identify abnormal . Palpate Head and Neck. Checking for lumps and bumps any lesions or tenderness. Check the ears. Use an Otoscope.

Head to Toe Assessment
E N D
Presentation Transcript
Head to Toe Assessment • https://www.youtube.com/watch?v=cP4zgb9H3Cg • Generalized patient assessment • Work from the head down • Know normal = identify abnormal
Palpate Head and Neck • Checking for lumps and bumps any lesions or tenderness
Check the ears • Use an Otoscope
Check Nose and Mouth • Is there redness, swelling, drainage, abnormal bumps, color, lesions
Pupil Check • PERRLA (pupils, equal, round, react to light, accommodate) • Accommodate – ability of eyes to focus on objects that are close up and faraway
Auscultation of Breath Sounds • Normal • Crackles- light crackling, bubbling • Rhonchi- coarse crackles • Wheezes- creaking, whistling, high pitched
Pulse Checks • Strength of pulse • 0 = absent • 1 = barely palpable • 2 = easily palpable • 3 = full • 4 = Bounding pulse
Capillary Refill • < 3 second Blood return • The rate at which blood refills empty capillaries • Indication of dehydration and peripheral perfusion
Skin Turgor • 1-3 second return • Used to assess the degree of fluid loss or dehydration
Peripheral Edema • Caused by fluid in the tissues tends to be dependent • 0 no edema • +1 Trace indentation rapid return to normal • +2 Mild indentation rebounds in a few seconds • +3 Moderate, 10-20 second to return to normal • +4 Severe, >30 second to return to normal
Bowel Sounds • Absent, Hyperactive, Hypoactive, Normal • To state absent you must listen for 5 min in each quadrant
Palpate the abdomen • To be done after listening to bowel sounds
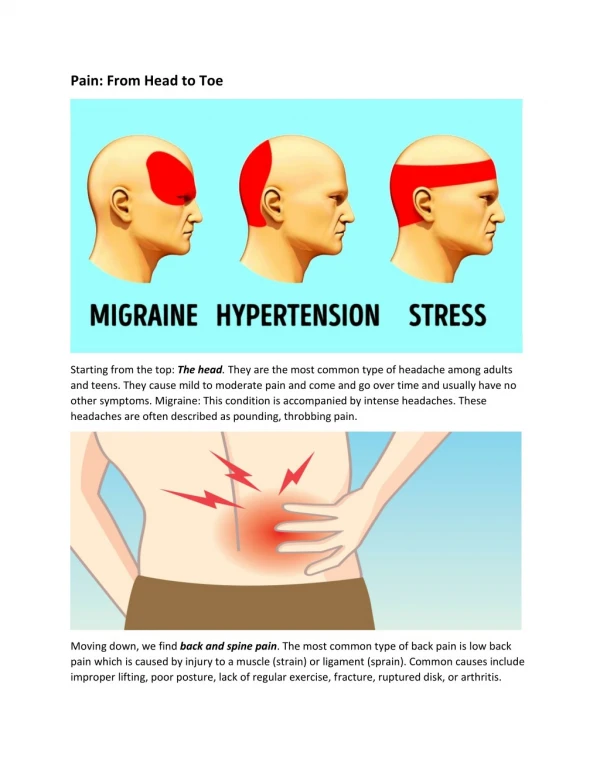
Pain • Location, duration, sensation, intensity • What makes it worse or better