Download
1 / 59
640 likes | 1.12k Views
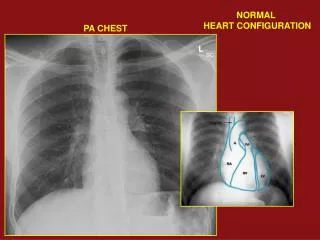
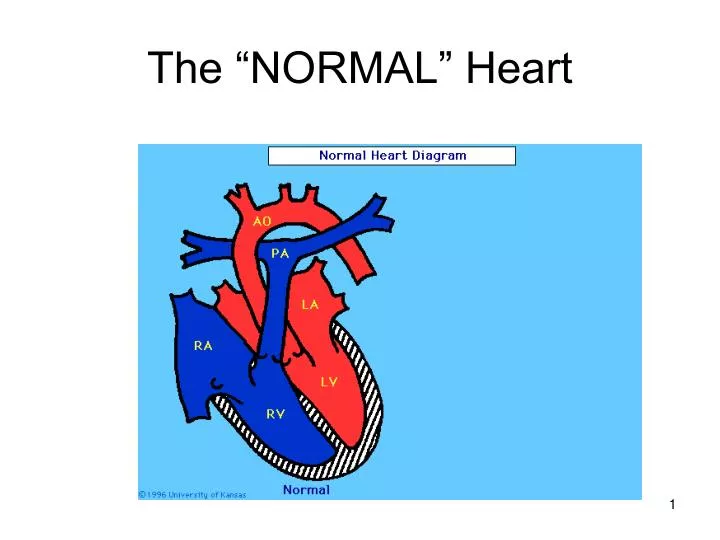
The “NORMAL” Heart. Cardiac Anatomy (cross section). Cardiac anatomy (external). Cardiac Auscultation. Cardiac Circulation. CYANOTIC Tetrology of Fallot (TOF) Transposition of the greater arteries (TGA). ACYANOTIC Atrial Septal Defect (ASD) Ventricular Septal Defect (VSD)

E N D
CYANOTIC Tetrology of Fallot (TOF) Transposition of the greater arteries (TGA) ACYANOTIC Atrial Septal Defect (ASD) Ventricular Septal Defect (VSD) Patent Ductus Arteriosus (PDA) Coarctation of the Aorta (COA) Cyanotic/ Acyanotic Defects
Atrial Septal Defect (ASD) An opening (hole) between the atria allowing blood from the higher pressure left atria to enter the lower pressure right atria. Degree of symptoms depends on the size of the hole. A child with a small ASD will have virtually no clinical symptoms but will have a significant murmur (the smallerthe hole, the louder the murmur).The smaller ASD can close spontaneously. The child with a large ASD will exhibit s/s of CHF.
Repair of ASD Repair can be performed in two ways • Open or closed heart surgery (depending on the type of defect and age of the patient) • A “umbrella” closure performed in the cardiac cath lab. A child with an unrepaired ASD does not require SBE prophylaxis.
Ventricular Septal Defect A opening (hole) between the right and left ventricle. VSD’s are the most common birth defect in children. Can range from a pin point sized hole to a large opening (virtually no septal wall present). Causes increased pulmonary blood flow and left to right shunting of blood flow, this increased flow cause increased work load on the RV predisposing the child to CHF.
A VSD is normally an acyanoticdefecthoweverIn very LARGE VSD’s ( there is virtually no septal wall) accompanied by significant congestive heart failure , cyanosis can be present.
Assessment of the child with a significant VSD Child will exhibit s/s of CHF: • Tachypnea, dyspnea • Poor growth = Failure To Thrive • Decreased fluid (formula) intake • Palpable cardiac thrill • Systolic murmur at lower sternal border
Medical treatment of a child with a VSD • Pharmacologic management of CHF. (Digoxin, Lasix). • Increased caloric intake to meet increased metabolic demands (increased BMR) • High calorie infant formula, commercial infant formula is 20kcal/oz, by adding less water/more concentrate or formula powder it will increase kcal/oz. Can go up to 30kcal/oz. • Synagis vaccine for RSV Sept- March
Surgical repair of VSD The vast majority of small VSD’s close spontaneously. The moderate-large will require open heart surgery to repair. • Age of repair depends on the degree of CHF. The child with a VSD will require SBE prophylaxis for life.
Nursing intervention (VSD) • Small frequent feeding of high caloric infant formula. • Must be monitored closely to be assured formula is being mixed correctly. Infant formula that is mixed improperly (to high a concentration) can be rapidly fatal. • Feeding log • Parental education • Medication administration • Teach parents s/s of CHF • Teach parents s/s infection (especially RSV Sept-March) • If possible once-twice a week phone contact in-between visits to the cardiologist for the infant with a moderate-large VSD. • Parental support • Provide referrals to support groups • Referrals and assistance to help with the high price of increased calorie formula (can be as high as $400 a month) • Frequent weights (outpatient- Minimum of wkly, inpatient - daily) • Referral to EI if child is not meeting developmental milestones
Coarctation of the Aorta (COA) A localized narrowing (coarctation) of the aorta Will cause increased pressure proximal to the defect (head and upper extremities) and decreased pressure to distal (body and lower extremities) Clinical Manifestations of COA (dependant on the degree of coarctation): • Increased BP • Bounding pulses in arms • Decreased BP in lower extremities • Decreased/Absent femoral pulses • Cool lower extremities
Degree of COA In infants with a significant COA, there can be s/s of CHF with rapid progression to the infant being critically ill with acidosis and hypotension. At this stage they will require intubation and Inotropic support until repair can be completed. With a milder degree of coarctation, the defect might not be diagnosed until it begins to produce symptoms (dizziness, headache, numbness in lower extremities, epitasis, syncope) Some children are not diagnosed until adolescence.
Surgical Repair of COA Can be achieved in 2 ways: • Balloon angioplasty of the coarcted area, done in the cardiac cath lab. A balloon catheter is threaded up to the are of the coarctation and opened in the coarcted area, in some cases just ballooning the area will work, in others a stent is needed to keep the aorta open. The potential for a re-COA is possible requiring a additional procedure. • Surgical repair (closed heart repair, no cardiopulmonary bypass is required). A resection and end to end anastamsois of the aorta is performed. A child with a COA will require SBE prophylaxis for life.
Patent Ductus Arterious (PDA) The failure of the fetal ductus arterious (the artery connecting the pulmonary artery and the aorta) to close within the first few weeks of life. In utero the PDA allows the blood to pass between the aorta and pulmonary artery by passing the lungs, it normally closes within the first 72 hrs -1 week after birth. Depending on how large the PDA is, when a large ductus stays open (patent), systemic BP becomes greater than pulmonary BP and the additional blood begins to shunt from the aorta across the ductus to the pulmonary artery, this is a left to right shunt. This shunt through the pulmonary artery through the lungs increases the workload of the left side of the heart and RV, which increases pulmonary vascular congestion and pulmonary vascular resistance which may cause increased right ventricular pressure and RV hypertrophy.
Treatment for PDA There are 3 treatments available to close the ductus: • Infusion of Indometicin (a prostaglandin inhibitor). • Surgical closure (closed heart) procedure is called a PDA ligation. Done via thoractomy. • Coil occlusion, a coil (spring like object) is inserted via a cardiac cath procedure and threaded to the level of the PDA, this coil occludes the PDA (and blood flow). It is successful with the small-moderate PDA. The child with a PDA will need SBE prophylaxis for oneyear after the duct is successfully closed.
Tetrology of Fallot Four defects • Pulmonic valve stenosis • Right Ventricular Hypertrophy (right ventricle wall is large and thick) • Ventricular Septal Defect (VSD) • Overriding Aorta (extends down to the level of the VSD)
TOF • Four defects are present: • Pulmonic Stenosis (stenosis of the pulmonary valve) • Right ventricular hypertrophy (RV wall is thick) • Ventricular Septal Defect (VSD) • Overriding Aorta (aorta is at the level of the VSD) These four defects combine to allow blood flow to bypass the lungs and enter the left side of the heart (and sending unoxygentated blood to the systemic circulation), this is called a Right to Left shunt.
TET SPELL They are hypercyanotic spells when there is an increase in the right to left shunting of blood (less oxygenated blood is getting to systemic circulation). TET spells can be precipitated by: • Crying • Cold • Defecation • Feedings
Treatment for TET Spells • Older unrepaired child will assume a squatting position (to decrease perfusion to lower extremities) This is rarely seen in the US, most children are repaired. • Put child in knee chest position to increase blood flow to upper extremities • IV Administration of Morphine sulfate • Administration of oxygen
Assessment of a child with unrepaired TOF • Clubbing of fingers/toes • Polycythemia (excess # of RBC’s) • Metabolic acidosis • Poor growth – FTT • Exercise- activity intolerance • Systolic murmur in pulmonic region • Cyanosis • O2 saturations as low as 50%
Treatment and Surgical Repair of TOF Degree of clinical manifestations and symptoms will depend on the degree of pulmonic stenosis. • For the child born with significant PS (the child born cyanotic) : • Oxygen administration • Correction of Metabolic acidosis • Immediate infusion of Prostaglandin E1 to keep PDA open to allow for mixing of blood. • Palliative surgery to improve oxygenation :Blalock taussig shunt or balloon septostomy to allow for mixing of blood • TET repair : closing of VSD, Resection or repair of pulmonary valve. Done anywhere from ages 6 months – 18 months depending on the degree of PS. • Requires open-heart surgery (cardiopulmonary bypass) • Child with TOF will require SBE prophylaxis for life.
Transposition of the greater arteries/vessels (TGA) • The greater vessels (aorta and pulmonary artery) positions are switched. • The pulmonary artery leaves from the left ventricle and the aorta leaves from the right ventricle. (normal heart :aorta from the left ventricle with oxygenated blood going to systemic circulation, pulmonary artery from the right ventricle with unoxygentated blood going to the lungs)
TGA • There must be an additional defect PDA , PFO or VSD to allow for the mixing of unoxygentated and oxygenated blood or the neonate will not receive any oxygenated blood into circulation. • This child is born cyanoticand needs immediate intervention to sustain life. • The patency of the PDA must be maintained with an infusion of Prostaglandin E1. • TGA is a ductal dependant defect – if the PDA closes the child will have severe hypoxia (O2 sats can be as low as 20%) severe cyanosis and acidosis. Death will follow very quickly. • The birth of a child with known or suspected TGA is a true medical emergency.
Treatment (at birth) for TGA • IV access • Intubation and mechanical ventilation • Infusion of PGE 1 at 0.1mg/kg/min to maintain patency of PDA • Pharmacologic paralysis and sedation • Correction of metabolic acidosis • Transfer to NICU with Pediatric cardiology services
Surgical treatment for TGA • Emergency procedure if child is too unstable for repair, if duct is closing and OR is not ready or surgery can not be performed immediately. • An artificial opening is made between the atria via a balloon septostomy (balloon catheter is threaded up to the atria and a hole is made) this is performed in the cardiac cath lab. It will allow the mixing of oxygenated and unoxygentated blood.
Arterial Switch for TGA • Should be done within the first few days (in rare cases weeks) after birth. • The aorta and pulmonary artery are resected at the level of the valves and reimplanted to their proper anatomical position. • Coronary arteries must also be resected. • During the post operative period (first 24 hours) the child is critically ill with the potential for :leaking around the multiple suture sites, arrhythmia's , hemorrhage and LV dysfunction. • After the initial postoperative period (with no significant complications ) there is a very good prognosis.
SBE prophylaxis • Current recommendation is Amoxicillin po 50mg/kg x1, 30mins prior to procedure • Recommendations change every couple years – check frequently
Congestive Heart Failure In CHD, CHF is usually caused by: • L to R shunting with increased pulmonary blood flow (large septal defects, both ASD & VSD) • Obstructive defects which impeded blood flow form the left ventricle (aortic stenosis) • Mixed defects: depending on the degree of mixing and pulmonary blood flow. CHF and cyanosis may occur together (TOF, TGA). One sided heart failure (as seen in adults) is rare in children, failure of one ventricle will almost always lead to failure of the other. Increased preload, decreased myocardial contraction, increased after load = impaired myocardial function CHF
Clinical Manifestations of CHF in children • Earliest s/s: tachycardia at rest HR >160
Digoxin • Pharmacologic classification: Cardiac glycoside • Therapeutic classification: Antiarrhytmic , inotropic • Indications: CHF, Atrial fibrillation, A flutter • Inotropic action: Increase force & velocity of myocardial contractions. In pts with CHF it increases contractile force and boosts cardiac output, improves systolic emptying. Depresses the SA node and prolongs conduction to the AV node. • How supplied: Pediatric Elixir 50mcg/ml Pediatric IV: 0.1mcg/ml
Special considerations for the use of Digoxin in the pediatric patient • Children have a poorly defined range of therapeutic levels, toxicity does not occur at the same levels that are considered toxic in the adult. Unless it is thought that a child is dig toxic, levels are not routinely done. • Children must use the same brand consistently. • Safety/accidental ingestions: Must be kept in a place that is physically impossible for a child to get to. A overdose of Digoxin will cause severe hypokalemia and rapid death (in some cases before it is even known that the child has taken it). • Treatment of overdose: Digibind, emesis induction, gastric lavage, administration of activated charcoal. • Metabolism: In hepatic system AND GUT. • Excretion: In renal system, dose must be adjusted in renal failure.
Total Digitalizing Dose (TDD) When starting Digoxin in a pediatric patient, children must be digitalized which means to give their loading dose in 3 doses, 8 hours apart
TDD 1st dose = ½ of TDD 2nd dose = ¼ of TDD, 8 hours after the first dose. EKG must be done before the 3rd dose. 3rd dose = ¼ of TDD, 8 hours after the 2nd dose.
Adverse reactions of Digoxin CNS • Fatigue • Muscle weakness • Agitation • Hallucinations • Headache • Dizziness Cardiovascular • Arrhythmias • Conduction disturbances: with or without AV block, PVC’s that may lead to increase ins severity of CHF. EENT • Yellow – green halo’s around visual images (hard to assess in pediatric pts) • Blurred vision • Light flashes • Photophobia GI • Anorexia • N/V/D