Download
1 / 28
320 likes | 601 Views
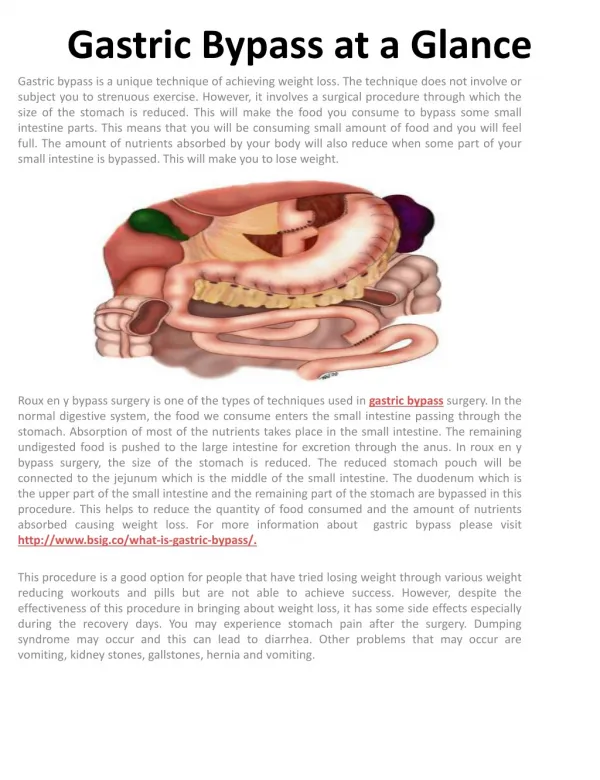
GI Complications of Gastric Bypass. Caroline R. Tadros , MD May 15 th 2013. Disclaimer.

E N D
GI Complications ofGastric Bypass Caroline R. Tadros, MD May 15th 2013
Disclaimer • This presentation has no commercial content, promotes no commercial vendor and has not been supported financially by any commercial vendor. I have not received financial remuneration from any commercial vendor related to this presentation.
Bariatric Procedures • Lap band http://www.nationalbariatric link.org • Sleeve Gastrectomy http://www.stfranciscare.org
Medical Complications of Roux-en-Y • Metabolic and nutritional derangements • Iron, calcium, vitamin B12, thiamine, and folate • Nephrolithiasis/Renal Failure1 • Hyperolaxuria • Post-operative hypoglycemia2,3 • Pancreatic nesidioblastosis (beta islet cell hypertrophy)
Medical Complications of Roux-en-Y • Change in bowel habits4 • Steatorrhea • Excessive fat intake • Lactose intolerance • Dumping Syndrome5 • Early6 • Onset within 15 minutes • Colicky abdominal pain, nausea, tachycardia, diarrhea • Usually self limited and resolves 7-12 weeks post operatively • Late • Onset 2-3 hours • Dizziness, fatigue, diaphoresis, and weakness
Mechanical Complications • Gastric Remnant Distention • Stomal Stenosis • Marginal Ulcers • Ulcers in excluded stomach • Cholelithiasis/Choledocholithiasis • Fistulas • Gastro-gastric • Gastro-intestinal
Gastric Remnant Distention • Etiology7,8 • paralytic ileus • distal mechanical obstruction • Iatrogenic injury to vagal fibers along the lesser curvature • Progressive distension can ultimately lead to rupture • Presentation9 • Abdominal pain • Hiccups • Shoulder pain • Abdominal distension • Tachycardia • Shortness of breath
Gastric Remnant Distention • Diagnosis • Left upper quadrant tympany • Gastric air bubble on imaging • Treatment10 • emergent decompression with a gastrostomy tube or percutaneous gastrostomy • Immediate operative exploration and decompression are required if percutaneous drainage is not feasible, or if perforation is suspected.
Stomal Stenosis • Etiology11 • Tissue ischemia • Increased tension on the gastro-jejunalanastamosis • Presentation • Several weeks postop • Nausea, vomiting, dysphagia, decreased oral intake, weight loss
Stomal Stenosis ( cont’d ) • Diagnosis • EGD • Upper GI series • Treatment12,13,14 • Endoscopic balloon dilation (perforation rate 3%) • Surgical revision (<0.05%)
Marginal Ulcers • Etiology 15,16 • Poor tissue perfusion due to tension or ischemia at the anastomosis • Presence of foreign material, such as staples or non-absorbable suture • Excess acid exposure in the gastric pouch due to gastro-gastric fistulas • Non-steroidal anti-inflammatory drug use
Marginal Ulcers • Etiology ( cont’d ) • Helicobacter pylori infection21-24 • High prevalence of H. pylori in bariatric patients • Preoperative treatment of HP decreased marginal ulcer rate form 6.8 to 2.4% • Smoking • Presentation • nausea, abdominal pain, bleeding and/or perforation
Treatment of Marginal Ulcers13 • Gastric acid suppression • Sucralfate • Discontinuation of NSAIDS • Smoking cessation • H. pylori therapy • Calcium channel blockers • Endoscopy/ IR embolization • Surgery (gastro-jejunostomy revision with truncalvagotomy)
Ulcers Within the Excluded Stomach • Endoscopy is limited due to the post surgical anatomy • Pancreatitis • If suspected operative management/intraoperative endoscopy25
Cholelithiasis • Rapid weight loss increases lithogenicity of bile20 • Frequency can be reduced with a six month course of ursodiol given post-operatively • Cholecystectomy at the time of bypass in those with symptomatic cholelithiasis26,27 • Cholecystectomy in asymptomatic patients is controversial
Choledocholithiasis • ERCP is of limited benefit • Typically requires PTC or surgery • Placement of a gastrostomy tube into bypassed stomach at the time of surgery or as necessary for pancreatobiliary/ duodenal access28,29
Internal Hernias • Occur in up to 5 % of patients undergoing laparoscopic bariatric surgery • Hernias through the transverse mesocolon are the most common and require operative repair30
Internal Hernias • Three potential areas of internal herniation31,15 • Mesenteric defect at the jejuno-jejunostomy • The space between the transverse mesocolon and Roux-limb mesentery (Peterson's hernias) • The defect in the transverse mesocolon if the Roux-limb is passed retrocolic
Internal Hernias ( cont’d ) • Intermittent, difficult to detect radiographically32,33 • If suspected, urgent surgical exploration is indicated • strangulated hernia may result in short bowel syndrome.
Mesenteric Swirl Sign Rev. Col. Bras. Cir. vol.39 no.3 Rio de Janeiro May/June 2012
Persistent Obesity • Failure to lose weight34 • rare and is often due to maladaptive eating patterns during the early postoperative period • Weight Regain34 • Occurs in up to 20% of patients, especially those with super-obesity (BMI>50 ) at the time of surgery
Differential Diagnosis of Weight Regain • Progressive noncompliant eating • development of a gastro-gastric fistula35,36,37 • gradual enlargement of the gastric pouch38,39 • dilatation of the gastro-jejunal anastomosis
Weight Regain Management • Fistula35,36,37 • UGIS if persistent or new onset GERD symptoms • surgical repair may be indicated • Dilatation of gastric pouch or the gastro-jejunal anastomosis • Repeated overdistention of the pouch from excessive food intake • No benefit of revisional surgery.
Excessive Weight Loss • Bacterial Overgrowth • Gastro-intestinal fistula
References • Oxalate nephropathy complicating Roux-en-Y Gastric Bypass: an underrecognized cause of irreversible renal failure. Nasr SH, D'Agati VD, Said SM, Stokes MB, Largoza MV, Radhakrishnan J, Markowitz GS Clin J Am SocNephrol. 2008;3(6):1676. • Hyperinsulinemichypoglycemia with nesidioblastosis after gastric-bypass surgery. Service GJ, Thompson GB, Service FJ, Andrews JC, Collazo-Clavell ML, Lloyd RV N Engl J Med. 2005;353(3):249. • Severe hypoglycaemia post-gastric bypass requiring partial pancreatectomy: evidence for inappropriate insulin secretion and pancreatic islet hyperplasia. Patti ME, McMahon G, Mun EC, Bitton A, Holst JJ, Goldsmith J, Hanto DW, Callery M, Arky R, Nose V, Bonner-Weir S, Goldfine AB Diabetologia. 2005;48(11):2236. • Bowel habits after bariatric surgery. Potoczna N, Harfmann S, Steffen R, Briggs R, Bieri N, Horber FF Obes Surg. 2008;18(10):1287. • Dumping syndrome: pathophysiology and treatment. Ukleja A NutrClinPract. 2005;20(5):517. • Change in effective circulating volume during experimental dumping syndrome. MATHEWS DH, LAWRENCE W Jr, POPPELL JW, VANAMEE P, RANDALL HT Surgery. 1960;48:185. • Jacobs, DO, Robinson, MK. Morbid obesity and operations for morbid obesity. In: Maingot's abdominal operations, 11th ed, Zinner, MJ, Ashley, SW (Eds), McGraw Hill, New York 2007. p. 471. • Effect of location and speed of diagnosis on anastomotic leak outcomes in 3828 gastric bypass cases.Lee S, Carmody B, Wolfe L, Demaria E, Kellum JM, Sugerman H, Maher JW J Gastrointest Surg. 2007;11(6):708. • Perforation in the bypassed stomach following laparoscopic Roux-en-Y gastric bypass. Papasavas PK, Yeaney WW, Caushaj PF, Keenan RJ, Landreneau RJ, GagnéDJObes Surg. 2003;13(5):797. • Perforation in the bypassed stomach following laparoscopic Roux-en-Y gastric bypass. Papasavas PK, Yeaney WW, Caushaj PF, Keenan RJ, Landreneau RJ, GagnéDJObes Surg. 2003;13(5):797. • Laparoscopic gastric bypass surgery: outcomes. Schneider BE, Villegas L, Blackburn GL, Mun EC, Critchlow JF, Jones DBJ LaparoendoscAdvSurg Tech A. 2003;13(4):247.
References • Endoscopic dilation of gastroesophageal anastomosis stricture after gastric bypass. Barba CA, Butensky MS, Lorenzo M, Newman R SurgEndosc. 2003;17(3):416. • Stomalcomplications of gastric bypass: incidence and outcome of therapy. Sanyal AJ, Sugerman HJ, Kellum JM, Engle KM, Wolfe L Am J Gastroenterol. 1992;87(9):1165. • Endoscopic management of stomal stenosis after Roux-en-Y gastric bypass. Go MR, Muscarella P 2nd, Needleman BJ, Cook CH, Melvin WS SurgEndosc. 2004;18(1):56. • Complications of the laparoscopic Roux-en-Y gastric bypass: 1,040 patients--what have we learned? Higa KD, Boone KB, Ho T Obes Surg. 2000;10(6):509. • Incidence and management of marginal ulceration after laparoscopic Roux-Y gastric bypass. Gumbs AA, Duffy AJ, Bell RL SurgObesRelat Dis. 2006;2(4):460. • Marginal ulcer after gastric bypass: a prospective 3-year study of 173 patients. Sapala JA, Wood MH, Sapala MA, Flake TM JrObes Surg. 1998;8(5):505. • Ulcer disease after gastric bypass surgery.Dallal RM, Bailey LA SurgObesRelat Dis. 2006;2(4):455. • Strictures following gastric stapling for morbid obesity. Results of endoscopic dilatation. Sataloff DM, Lieber CP, Seinige Am Surg. 1990;56(3):167. • Changes in gallbladder bile composition following gallstone formation and weight reduction. Shiffman ML, Sugerman HJ, Kellum JM, Moore EW Gastroenterology. 1992;103(1):214. • Marginal ulceration after laparoscopic gastric bypass: an analysis of predisposing factors in 260 patients. Rasmussen JJ, Fuller W, Ali MR SurgEndosc. 2007;21(7):1090. • Flexible endoscopy in the management of patients undergoing Roux-en-Y gastric bypass. Schirmer B, Erenoglu C, Miller A Obes Surg. 2002;12(5):634. • Endoscopic and histologic findings of the foregut in 426 patients with morbid obesity. Csendes A, Burgos AM, Smok G, Beltran M Obes Surg. 2007;17(1):28. • Early effects of Helicobacter pylori infection in patients undergoing bariatric surgery. Ramaswamy A, Lin E, Ramshaw BJ, Smith CD Arch Surg. 2004;139(10):1094. • Bleeding Duodenal Ulcer After Roux-en-Y Gastric Bypass SurgeryMarc Zerev, , MD, FRCSC;Lee B. Sigmon, BS; Timothy S. Kuwada, MD; B. Todd Heniford, MD; Ronald F. Sing, DOJ Am Osteopath Assoc January 1, 2008 vol. 108 no. 1 25-27
References • Is routine cholecystectomy required during laparoscopic gastric bypass? Villegas L, Schneider B, Provost D, Chang C, Scott D, Sims T, Hill L, Hynan L, Jones D Obes Surg. 2004;14(2):206. • Elective cholecystectomy during laparoscopic Roux-en-Y gastric bypass: is it worth the wait? Hamad GG, Ikramuddin S, Gourash WF, Schauer PR Obes Surg. 2003;13(1):76. • Surgical gastrostomy placement as access for diagnostic and therapeutic ERCP. Baron TH, Vickers SM GastrointestEndosc. 1998;48(6):640. • ERCP in patients with long-limb Roux-en-Y gastrojejunostomy and intact papilla. Wright BE, Cass OW, Freeman ML GastrointestEndosc. 2002;56(2):225. • Small bowel obstruction and internal hernias after laparoscopic Roux-en-Y gastric bypass. Champion JK, Williams M Obes Surg. 2003;13(4):596. • Laparoscopic versus open gastric bypass: a randomized study of outcomes, quality of life, and costs. Nguyen NT, Goldman C, Rosenquist CJ, Arango A, Cole CJ, Lee SJ, Wolfe BM Ann Surg. 2001;234(3):279. • Sensitivity and specificity of eight CT signs in the preoperative diagnosis of internal mesenteric hernia following Roux-en-Y gastric bypass surgery. Iannuccilli JD, Grand D, Murphy BL, Evangelista P, Roye GD, Mayo-Smith W ClinRadiol. 2009;64(4):373. • Internal hernia after gastric bypass: sensitivity and specificity of seven CT signs with surgical correlation and controls.Lockhart ME, Tessler FN, Canon CL, Smith JK, Larrison MC, Fineberg NS, Roy BP, Clements RHAJR Am J Roentgenol. 2007;188(3):745. • Binge eating among gastric bypass patients at long-term follow-up. Kalarchian MA, Marcus MD, Wilson GT, Labouvie EW, Brolin RE, LaMarca LB Obes Surg. 2002;12(2):270. • Gastro-gastric fistulas and marginal ulcers in gastric bypass procedures for weight reduction. Capella JF, Capella RF Obes Surg. 1999;9(1):22. • Management of gastrogastric fistulas after divided Roux-en-Y gastric bypass surgery for morbid obesity: analysis of 1,292 consecutive patients and review of literature. Carrodeguas L, Szomstein S, Soto F, Whipple O, Simpfendorfer C, Gonzalvo JP, Villares A, Zundel N, Rosenthal R SurgObesRelat Dis. 2005;1(5):467. • Stomalulcer after gastric bypass.MacLean LD, Rhode BM, Nohr C, Katz S, McLean AP J Am Coll Surg. 1997;185(1):1. • Treatment of dilated gastrojejunostomy with sclerotherapy. Spaulding L Obes Surg. 2003;13(2):254. • Peroralendoscopic reduction of dilated gastrojejunal anastomosis after Roux-en-Y gastric bypass: a possible new option for patients with weight regain. Thompson CC, Slattery J, Bundga ME, Lautz DB SurgEndosc. 2006;20(11):1744.