Download
1 / 34
390 likes | 1.65k Views
Brucell Weil Felix test Widal test. Brucell. Gram negative small coccobacilli . Non- motile. None encapsulated. Fastidious, need special media with CO 2 and anaerobic condition for growth these media called as Castenada media .

E N D
Gram negative small coccobacilli. • Non- motile. • None encapsulated. • Fastidious, need special media with CO2 and anaerobic condition for growth these media called as Castenada media. • facultative intracellular parasites causing chronic disease • Cause brucellosis disease or undulating fever.
Species of Brucella: • Brucellaabortus • Brucellamelitinsis • Brucellabovis • Brucellasuis.
Mode of transmission: • Brucellosis is a zoonotic disease transmitted by: • Ingesting infected food by Brucellabacteria. • Direct contact with infected animals. • Inhalation of aerosols. • Consumption of unpasteurized milk products. • Transmission from human to human, through sexual contact or from mother to child, is rare but possible.[1]
Symptoms: • Signs and symptoms are similar to those of the flu and include: • Fever • Chills • Sweats • Weakness • Fatigue • Joint, muscle and back pain • Headache • Brucellosis symptoms may disappear for weeks or months and then return. In some people, brucellosis becomes chronic, with symptoms persisting for years, even after treatment. Long-term signs and symptoms include fatigue, fevers, arthritis and spondylitis — an inflammatory arthritis that affects the spine and adjacent joints. • The infection can usually be treated successfully with antibiotics. Treatment takes several weeks, however, and relapses are common.
Diagnosis : • Blood culture in first week of infection. • Brucella is isolated from a blood culture on Castenada medium. Prolonged incubation (up to 6 weeks) may be required as they're slow-growing, but on modern automated machines the cultures often show positive results within seven days. On Gram stain they appear as dense clumps of Gram-negative coccobacilli and are exceedingly difficult to see. • Animal inoculation test. • Serology test. • Serology for brucellosis is a blood test to look for antibodies against Brucella, the bacteria that causes the disease brucellosis. The blood is then tested in a laboratory to look for antibodies. For Brucella, the serum agglutination test (SAT) is the simplest and most widely used testing method. This test done after 2 weeks (10 days) of fever.
The CDC/Council of State and Territorial Epidemiologists case definition for human brucellosis states that the laboratory criteria for diagnosis includes • 1) Isolation of Brucella species from a clinical specimen, • 2) Four-fold or greater rise in Brucella agglutination titer between acute- and convalescent-phase serum specimens drawn >2 weeks apart and studied at the same laboratory, or • 3) Demonstration by immunofluorescence of Brucella species in a clinical specimen.
Normal results: • A normal result shows no antibodies to Brucella. However, during the first few days to weeks of exposure to an antigen, there may be very little antibody production. As brucellosis progresses, more antibodies will be present. If the health care provider suspects brucellosis, you may need to have the test repeated 10 days to 2 weeks after the first test to watch for this rise. • Negative to a titer of > or =1:40 can be seen in the normal, healthy population. A titer of > or =1:80 is often considered clinically significant;(1) however, a 4-fold or greater increase in titer between acute and convalescent phase sera is required to diagnose acute infection. • Prozone phenomena: • The presence of high antibody titer that lead to Ag block and hence false negative results are obtained. Dilution will resolve this problem.
Note: • A normal (negative) result usually means you have not come in contact with the bacteria that causes brucellosis. However, this test may not detect the disease at an early stage. Your doctor may have you come back for another test in 10 days to 3 weeks. • Brucellaantibody have long lifespan may reach one year. • Infection with other bacteria, such as Yersinia , Francisella , and Vibrio , and certain immunizations can cause false-positive results. • Normal value ranges may vary slightly among different laboratories. Some labs use different measurements or test different samples. Talk to your doctor about the meaning of your specific test results. • An abnormal (positive) results usually means you have come in contact with the bacteria that causes brucellosis. However, this does not mean that you have an active infection. Your doctor will repeat the test after a few weeks to see if the test result increases. This is more likely to be a sign of a current infection.
Rickettsia • Obligately intracellular • grown in embryonated eggs or tissue culture • Gram-negative • Small, pleomorphic coccobacilli • Transmitted by arthropod vectors (ticks, lice, fleas, mites, chiggers). • Include the genera Rickettsiae, Ehrlichia, Orientia, and Coxiella. • zoonotic pathogens cause infections that disseminate in the blood to many organs.
Complications: • Lymphocytosis • Leukopenia • Thrombocytopenia • Anemia, in some cases hemoglobin may increase as result of hemoconcentration. • Urine analysis will show high RBCs, cast may be present, high protein . • Increase blood urea and creatinine.
INVESTIGATIONS • PCR – Amplification of O tsutsugamushi DNA from the blood of febrile patients. SEROLOGICAL TESTS such as • Indirect Flourescent antibody test (IFA) test ( Titer ≥ 1: 200 ), • the Complement Fixation Test. • The Weil Felix Test • Scrub IgM ELISA Test: Highly specific test
Weil Felix test • Reckettsial infection (typhus fever) will cause heterolphilic antibodies that agglutinate some strains of Proteus. • The agglutination reactions, the basis of the test is the sharing of an Alkali stable carbohydrate antigen of rickettsia and by certain strains of Proteus. • Slide and tube method. • Test is negative in rickettsialpox, • False positive reaction may occur in urinary or other Proteus infections.
Typhus group rickettsiae • (Rickettsia prowazekii, R. typhi) react with P. vulgaris OX19, • scrub typhus (Orientiatsutsugamushi) reacts with P. mirabilis OXK. T • thespotted fever group rickettsiae (R. rickettsii, R. africae, R. japonica, etc.) react with P. vulgaris OX2 and OX19, to varying degrees, depending on the species.[2]
Diagnosis of Rickettsiosis(typhus fever ) : • difficult to diagnose both clinically and in the laboratory. • Cultivation requires viable eukaryotic host cells, such as antibiotic-free cell cultures, embryonated eggs, and susceptible animals. • Confirmation of the diagnosis requires comparison of acute- and convalescent-phase serum antibody titers. • If OX-19 test is positive, this result is due to infection with Proteus or Rickettsia. • The Weil–Felix test suffers from poor sensitivity and specificity, with a recent study showing an overall sensitivity as low as 33% and specificity of 46%. • As a result, it has largely been supplanted by other methods of serology, including indirect immunofluorescenceantibody (IFA) testing, which is the gold standard.
Slide method (Laboratory Test) On a solid surface (glass slide, tile, card), a small amount (50–100 μL) of the patient’s serum is placed. A single drop of the desired antigen is added, and the resulting suspension is mixed and then rotated for one minute. Visible agglutination is indicative of a positive result, and corresponds roughly to a titre of 1:20. Positive results can be further titrated using the tube method, which is more labour-intensive.
Tube method (Laboratory Test) Using 0.25% phenol saline as a diluent, a series of tubes containing twofold dilutions of patient serum are made with a final volume of 1 mL. A drop of antigen suspension is added to each tube The mixture is incubated at 50–55 °C for 4–6 hours. A positive tube would show visible flocculation or granulation, which is accentuated when the tube is gently agitated. The titer corresponds to the most dilute tube in the series that still shows positivity. Generally, a titre of ≥1:320 is considered diagnostic.
To differentiate between Proteus infection and Rickettsial infection:
Use to diagnosis of typhoid fever which caused by Salmonella. • In diagnosis of typhoid fever, patient serum is tested for salmonella O and H antibodies against Ag suspension. • The test is done after 2-3 weeks of infection or after 10 days of fever. • There are two species of Salmonella : • Salmonella typhi • Salmonella paratyphi • S. paratyphi A • S. paratyphi B • S. paratyphi C
Both typhi and paratyphi have two types of antigen: • Somatic ( O ) antigen, and that is thermostable. • Flagellar( H ) antigen, and that is thermolabile. • Salmonella can be isolated from GIT, urine, blood, bile, bone marrow, sputum, food products, and milk. • The confirmatory test for Salmonella is stool culture at the first week of infection.
H( flagel) antigens O (somatic) antigens Vi (Virulence) capsular polysaccharide antigens Antigenic structure of Salmonella
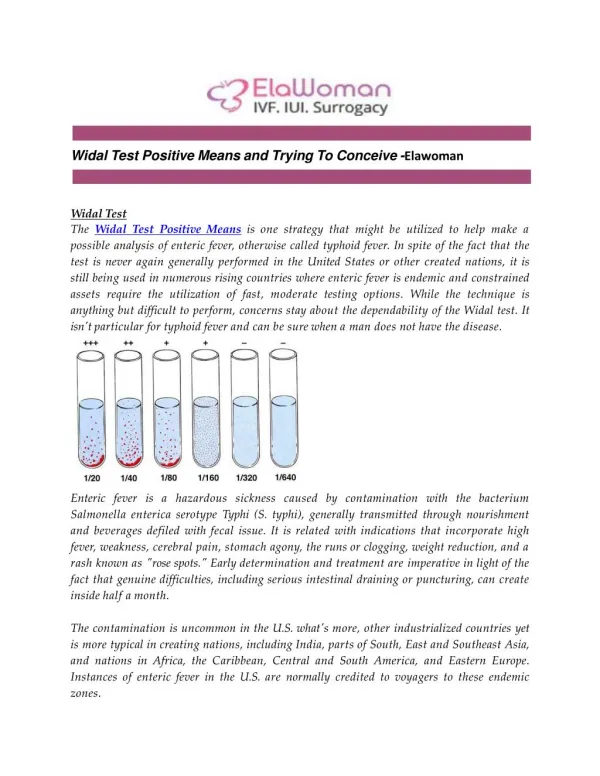
Principle of test: Patients suffering from enteric fever would possess antibodies in their sera which can react and agglutinate serial doubling dilutions of killed colored Salmonella antigens in a tube agglutination test.
Procedures: Slide method A slide widal test is more popular among diagnostic laboratories as it gives rapid results. Qualitative test: One drop each of undiluted patients’ serum samples for the four antigens are placed on the circled card and one drop of each of the four Salmonella antigens are added separately and gently rotated for one minute. Appearance of agglutination gives qualitative results. To know the titer for each of the antigens, the test is repeated with dilutions of serum.
Quatitative test: 80 μl, 40 μl, 20 μl, 10 μl and 5 μl of patient’s serum each for the four antigens are placed on the circled card. To each series of serum specimen, one drop of specific antigen is added to each, mixed and rotated for one minute. Agglutination in each of these is noted. 80 μl corresponds to 1/20 dilution, 40 μl to 1/40, 20 μl to 1/80, 10 μl to 1/160 and 5 μl corresponds to 1/320 titre.
Procedures: Incubated in water bath at 370C overnight • Tube method:
Reading the results: The control tubes must be examined first, where they should give no agglutination. The agglutination of O antigen appears as a “matt” or “carpet” at the bottom. Agglutination of H antigens appears loose, wooly or cottony. The highest dilution of serum that produces a positive agglutination is taken as titer. The titers for all the antigens are noted.
Other Methods: • Typhiod Rapid IgM-Assay • Detects specific IgM and IgG antibodies to S. Typhi • PCR • The PCR technology has an unparalleled sensitivity and specificity for the diagnosis of typhoid
Rapid IgM Kit HBSAG HCV HIV HPYLORI MALARIA TYPHIDOT TOXOPLASMA