Download
1 / 34
360 likes | 582 Views
PAVE ing the way to improved limb preservation. Jeffrey M. Robbins, DPM Director, Podiatry Service VACO November 17, 2012. Learning Objectives. At the conclusion of this activity, the participant will be able to:

E N D
PAVE ingthe way to improved limb preservation Jeffrey M. Robbins, DPM Director, Podiatry Service VACO November 17, 2012
Learning Objectives At the conclusion of this activity, the participant will be able to: • A. Describe the importance of the Prevention of Amputation in Veterans EverywhereProgram • B. List the components of calculating foot risk score • C. Discuss the morbidity and mortality associated with first onset diabetic ulceration
Disclosures • Jeffrey M. Robbins, DPM has no financial interest or relationships to disclose.
“Every system is perfectly designed to get the results it gets.” Paul Bataldan
Veterans Medical Programs Amendments of 1992 (PL102-405) • Emphasized importance of highest quality amputee care • Identified veterans with amputation as a special disability group • Chartered the Advisory Committee on Prosthetics and Special Disabilities Programs
PAVE • 1.PURPOSE: This Veterans Health Administration (VHA) Directive defines the scope of the care and treatment provided to veteran patients at risk of primary or secondary limb loss. This is accomplish through the Prevention of Amputation in Veterans Everywhere (PAVE) Program
1993 PACT Program Launched • Developed to meet the changing needs of veterans • more neuropathy, PVD and diabetes • fewer traumatic amputations • New issues in 2006 with returning OEF/OIF Vets • Established a model of care to prevent or delay amputations • Proactive early identification of “at risk” populations • Especially veterans with diabetes • Track from date of entry to discharge back to the community
Policy • 3.POLICY: It is VHA policy that the PAVE program be established at all VA medical centers. The program will at a minimum provide for
Policy: Screen/Risk Assess/Refer • 1. Screeningof at-risk populations • 2. Identification of high risk patients • 3. Timelyand appropriately referral
Policy: Mental Health Consult • 4. Each patient who has suffered an amputation should be offered a visit by their mental health consultation team, to assess coping and provide support as needed either in an individual or group format. (This approach avoids stigmatizing anyone as being singled out as having mental or emotional issues and also minimizes the potential for missing someone who is 'suffering in silence")
Policy: Identify and Track • 5. Development of a system to identify and track patients with amputation or those at risk for amputation. • NOTE: (The VACO Patient Care Services PAVE ProClarity Cubes are an acceptable resource from which to develop such a system)
Policy: Champion • 6. A PAVE coordinator to provide for • (a) organizational support for the PAVE team, • (b) communication conduit between administration and PAVE/Amputee clinic team providers, • (c) a smooth transition of the DOD patient into the VA system
Policy: Interdisciplinary Committee • 7. A PAVE Committee should be established to coordinate efforts to address the primary amputation prevention needs of “at risk” patients, and the secondary amputation prevention needs for those patients who have already suffered an amputation. This includes patients who had their amputations outside the VA system of care (e.g. OEF/OIF, private hospital, etc). This may be accomplished by the PAVE coordinators incorporating their efforts in existing primary amputation prevention committees within the medical centers.
VA Central Office PAVE Oversight Committee • The field based PAVE Oversight Committee made up of clinical leaders from endocrinology/diabetes, podiatry, PM&R, Prosthetics, nursing the VISN’s, OQPresponsible for recommendations for data collection and analyses to permit program evaluation of the screening, surveillance, salvage, and rehabilitative components of the PAVE program, including the following
Policy • 1. Identification of veterans at risk for or who have sustained an amputation • Age adjusted and stratified rates of major (AKA and BKA) and minor amputations, and lower extremity non-venous ulcers • Patient knowledge and performance of recommended self foot care practices, and satisfaction with foot care. • VISN and Facility adherence to the PAVEDirective with respect to formal policies and coordination strategies
Proposed: Program Improvement • The PAVE committee will use these analyses to identify best practices from the field, and to make recommendations to achieve excellence in patient centered care to the PAVE Oversight Committee for program improvements • Recommendations RE: self foot care behaviors
Opportunity: SFCB • Let patients know that these self care behaviors are important to their provider • Allows the provider to reinforce the behavior in a quick and efficient manner.
CPRS Follow-up on Self Foot Care Behaviors • Are you or your caregiver having an problems inspecting your feet every day? • Can’t see or can’t reach • Can we offer you a mirror, etc. • Are you or a caregiver having an problems washing your feet? • Can’t see or can’t reach • Can we offer you a sponge on a stick, etc. • Do you walk barefoot?
Policy: Defines Responsibility • A. The Network Director is responsible for: • B. Medical Center Director • C. Chief of Staff • D. PAVE Coordinator
Program Components • Directive provides recommendations for; • Foot Checks • Foot Examinations • Risk Score assignments • Referral strategy • Provides guidelines not mandates!
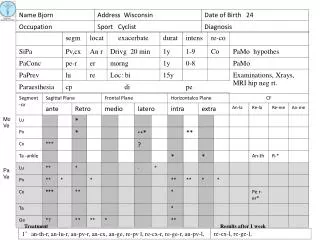
Foot Screening • 1. FOOT Screening • This would involve: • a. Visual inspection of the skin surface for any lesions, deformities, color or temperature changes or ulcers; • b. Screening for circulation, i.e., the palpation of pedal pulses in the foot; and • c. Sensory testing using a Semmes-Weinstein 5.07 monofilament to check for loss of protective sensation.
Foot Examination • 2. FOOT Examination • This involves a more in-depth evaluation of the foot’s circulation and sensation as well as foot deformities. During this examination, patients are evaluated by a "foot care specialist," e.g., Prevention of Amputation in Veterans Everywhere (PAVE) program member, vascular surgeon, podiatrist, or other health care professional demonstrating appropriate education, training, competencies and licensure necessary to provide such care
Foot Risk Score • RISK ASSESSMENT LEVEL • "At-risk" is defined as patients with diabetes, peripheralvasculardiseaseand/or endstagerenaldisease, who are considered highly susceptible to develop foot ulcers. • “High Risk” is defined as any patient who has had an amputation for any reason, and patients with a foot risk score of 2 or 3.
Foot Risk Score • a. Level 0, Normal Risk. These patients have no evidence of sensory loss, diminished circulation, , ulceration, or history of ulceration or amputation. Patients with diabetes should receive foot care education and annual foot screening. These patients do not require therapeutic footwear. • b. Level 1, Low Risk . These individuals demonstrate one or both of the following • Foot deformity or minor foot infection (and a diagnosis of diabetes). • Patient education, preventative care and annual foot screening are required. The patients in this category and the following two categories (Level 2 and Level 3) should not walk barefoot. Special attention is to be directed to shoe style and fit. These individuals do not need therapeutic footwear.
Foot Risk Score • c. Level 2, Moderate Risk. These individuals demonstrate sensoryloss (inability to perceive the Semmes-Weinstein 5.07 monofilament) and may have one additional finding below. • Diminished circulation as evidenced by absent or weakly palpable pulses, (this would require follow-up examination to determine level of vascular disease before a final risk score can be determined) • Foot deformity or minor foot infection (and a diagnosis of diabetes).
Foot Risk Score • These individuals require: • therapeutic footwear and orthoses to accommodate foot deformities, to compensate for soft tissue atrophy, and to evenly distribute plantar foot pressures. • Patient education, regular preventive foot examination and care in podiatry or other foot care specialty clinic. • Patient health education (PHE) must include the implications of sensory loss and the importance of daily foot inspections. • NOTE:May require Diabetic Socks and Depth Inlay Shoes based on clinical judgment.
Foot Risk Score • Level 3, High Risk. These individuals demonstrate peripheral neuropathy with sensory loss (inability to perceive the Semmes-Weinstein 5.07 monofilament) anddiminishedcirculationandfoot deformity or minor foot infection (and a diagnosis of diabetes). • or any of the following by itself • Prior ulcer, Osteomyelitis or history of prior amputation • Severe PVD (intermittentclaudication, dependent rubor with pallor on elevation, or critical limb ischemia manifested by rest pain, ulceration or gangrene., • Charcot’s joint disease with foot deformity. • End Stage Renal Disease • These individuals are at highest risk of lower extremity events. Individuals in this category require extra depth footwear with soft molded inserts. They may require custom molded shoes and braces (e.g., double upright brace, patella tendon bearing orthoses, etc.). More frequent clinic visits are required with careful observation, regular preventive foot care, and footwear modifications. • NOTE:May require Diabetic Socks, Depth Inlay Shoes or Custom-Molded Orthopedic Shoes based on clinical judgment.
Who are our patients? • Patients 1,514,197 • Age Avg69.3 • Amputation Last 18 Mos7,176 • HxAmputation Last 10 Years 45,134 • HxCharcot Foot 4,794 • HxDiabetes 1,260,752 • HxESRD 18,385 • Hx Foot Deformity or Surgery 377,053 • HxGangrene 7,648 • HxNeuropathy 322,610 • HxNon-Healing Ulcer 58,440 • HxOsteomyelitis 13,105 • HxPVD 300,765 • HxPVD Surgery 9,007 • Hx Smoking % 20.12%
Summary • Best system anywhere but we need to do even better • We have been following patient centered medical home principals • Must do better to convince patients to engage in self foot care practices. • PAVE and ASoC coordination, co-operation should help us improve the system of care.