Download
1 / 15
160 likes | 494 Views
Sarah E. French, MD ACP MS/LA Regional Meeting May 7, 2010. Hypersomnolence as Presenting Symptom of Thalamic Infarction. Introduction. Hypersomnolence has a broad differential diagnosis including ingestions, metabolic disturbances, sleep disorders, and neurologic syndromes.

E N D
Sarah E. French, MD ACP MS/LA Regional Meeting May 7, 2010 Hypersomnolence as Presenting Symptom of Thalamic Infarction
Introduction Hypersomnolence has a broad differential diagnosis including ingestions, metabolic disturbances, sleep disorders, and neurologic syndromes. With no accompanying gaze disturbances or other neurologic deficits, diagnosing a thalamic infartction may be challenging.
Patient Presentation Patient is 45-year-old man with hypertension, dyslipidemia, tobacco use and depression who was brought to the hospital by his wife for increased somnolence. Previous day he had attended a funeral, returned home and went to bed.
Patient Presentation (cont'd) At 3 am, his wife tried to wake him up because he was snoring louder than usual but could not get him to awaken fully. Later that morning she could only get him to wake up for a few minutes at a time and to follow simple commands. His wife denied any neurological deficits, seizure activity, ingestions, or falls.
Physical Examination Patient appeared asleep but was arousable to voice. He was able to answer yes/no questions and follow simple commands. He quickly fell back to sleep without stimulation.
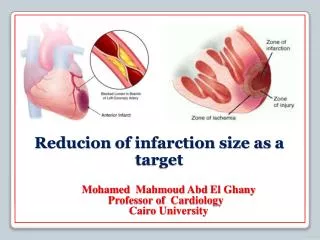
Initial Work-up Labwork including CBC, chem 8, LFTs, TSH, cortisol, urine drug screen, and serum alcohol level was normal. Room air ABG was normal. CT head showed remote lacunar infarctions in left caudate and anterior aspect of both thalami but no acute intracranial abnormalities.
Further Work-up Neurology was consulted. CT angiogram of head and neck demonstrated no intracranial stenosis/lesions or aneurysms. EEG had no epileptiform discharges. Psychiatry was consulted and felt that patient's symptoms were not due to his depression.
Further Work-up (cont'd) Patient began to have periods of wakefulness lasting up to 4 hours. Patient had no memory of preceding 2-3 days, including the funeral he had attended the day before admission. MRI of brain revealed acute infarction of left internal capsule and anterior thalamus.
Further Work-up (cont'd) Hypercoagulable work-up was initiated and was negative except for elevated fibrinogen. On hospital day 7, patient was having longer periods of wakefulness and discharged home.
Case Discussion • Paramedian thalamic infarction has been associated with triad of hypersomnolence, memory deficits and vertical gaze palsy. • However, many patients with paramedian thalamic infarction do not present with the full triad. Nagaratnam, N; et al. Syndrome of downward gaze paralysis, anemia and hypersomnolence. Postgraduate Medical Journal (1989) 65, 840-842.
Case Discussion • In one case series, CT head revealed no signs of haemorrhagic infarct. • Four-vessel cerebral angiography failed to reveal an underlying vascular anomaly or pathology. • All patients in the series were found to have ischaemic lesions in the paramedian thalamus on MRI. Lovblad, KO; et al. MRI of paramedian thalamic stroke with sleep disturbance. Neuroradiology (1997) 39: 693-698.
Case Discussion • Sleep studies have shown an increased sleep duration with predominance of superficial sleep stages, increased sleep fragmentation, and decreased sleep spindles. • Post-stroke hypersomnia improves considerably within months but the sleep EEG changes may remain unchanged for years. Hermann, D; et al. Evolution of Neurological, Neuropsychological and Sleep-Wake Disturbances After Paramedian Thalamic Stroke. Stroke. 2008;39:62-68.
Case Discussion • Right-sided infarcts have significantly better long-term recovery. • Left-sided and bilateral infarcts present more regularly with deficits in executive functions and memory. Hermann, D; et al. Evolution of Neurological, Neuropsychological and Sleep-Wake Disturbances After Paramedian Thalamic Stroke. Stroke. 2008;39:62-68.
Case discussion • Overall, the prognosis is fair. • In most case series, only one or less actually died. • Memory, hypersomnia and vertical gaze paresis improved with time and did not hinder patients in their activities. Gentilini, M; et al. Bilateral paramedian thalamic artery infarcts: report of eight cases. J NeurolNeurosurg Psychiatry 1987 50: 900-909.
References • Nagaratnam, N; et al. Syndrome of downward gaze paralysis, anemia and hypersomnolence. Postgraduate Medical Journal (1989) 65, 840-842. • Hermann, D; et al. Evolution of Neurological, Neuropsychological and Sleep-Wake Disturbances After Paramedian Thalamic Stroke. Stroke. 2008;39:62-68. • Lovblad, KO; et al. MRI of paramedian thalamic stroke with sleep disturbance. Neuroradiology (1997) 39: 693-698. • Gentilini, M; et al. Bilateral paramedian thalamic artery infarcts: report of eight cases. J NeurolNeurosurg Psychiatry 1987 50: 900-909.