Download
1 / 24
310 likes | 3.9k Views
Benign diseases of vulva . Dr. R. Elgantri Associated prof. Department of Obs. & Gyn. Alfath University. Benign disease of vulva. Anatomical consideration Vulval skin comprises stratified squamous epithelium as in other parts of body

E N D
Benign diseases of vulva Dr. R. Elgantri Associated prof. Department of Obs. & Gyn. Alfath University
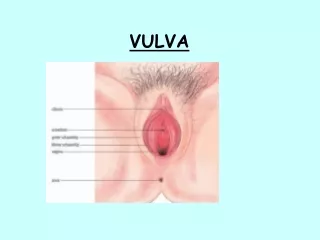
Benign disease of vulva Anatomical consideration Vulval skin comprises stratified squamous epithelium as in other parts of body The mons pubis and labia majora contain fat, sebaceous, apocrine and eccrine sweat glands and blood vessels , which can develop varicosities Labia minora are rich in sebaceous gland, contain few sweat gland but no hair follicles The epithelium of the vestibule is neither pigmented nor keratinized, but contain eccrine glands. These glands and epithelial appendages are a source of lumps
Deep to the posterior parts of labia majora are the Bartholin’s gland or greater vestibular glands, whose ducts open into the posterior part of the vagina, just behind the midpoint and superficial to hymenal ring. The glands and ducts can be the site of infection or cyst formation Presenting features The usual presenting features are: vulval pruritus vulval pain, burning lump superficial dyspareunia white discoloration of vulva
Examination should include examination external genitalia and the whole genital tract Vulval biopsy Is necessary to confirm the diagnosis if not clear and to see whether is pre-invasive or invasive Colposcopy of the vulva is helpful to determine area from which biopsy should be taken
Non-neoplastic epithelial disease Lichen sclerosus squamous cell hyperplasia other dermatomes contact and allergic dermatitis seborrhoeic dermatitis psoriasis lichen planus Hid adenitis supperutiva Behest's disease
Lichen sclerosis Is characterized by epithelial thinning, inflammation and distinctive histological changes in the dermis The incidence is unknown It can affect both sexes and can occur at any age Typically found in anogenital region in postmenopausal women It can be asymptomatic but the most common presentations are: intractable itching (pruritus vulvae) vaginal soreness dyspareunia
Etiology unknown Signs: - crinkled or parchment-like appearance that usually extends around the anal area in a figure of eight configuration - atrophy of labia minora - constriction the vaginal orifice - adhesion and telangiectasia
Prognosis Can occur in children and in2/3rd of cases the lesions will clear at puberty In adults, it is a chronic condition that can be considered as pre-malignant (the rate progression varies from0 to 9%) Management The aims of management are to control the symptoms and to detect changes suggestive of malignant change
General measures Reassurance; that it is well recognized condition and can be satisfactorily controlled with simple measures Bland emollient should be used liberally and can provide significant relief Topical steroids Clobetasol propionate provide significant relief than local testosterone and petroleum jelly
Surgery In general surgery should be avoided unless there is malignant change
Lichen planus It can be acute or chronic condition affecting the skin or mucous membranes or both On keratinized skin, lichen planus is characterized by flat-topped , shiny papules On the vulva, the appearance ranges from delicate, white reticulated papules to an erosive, desquamated process Incidence It is uncommon Etiology unknown
Prognosis The lesions tend to disappear after weeks or months Erosive lesions heal poorly and may be pre-malignant Diagnosis: is confirmed by biopsy Treatment Topical steroid Short courses of systemic corticosteroids
Inflammatory dermatomes Can be classified as either: contact dermatitis primary irritant dermatitis It is difficult to differentiate between the two Typical findings are: diffuse reddening of the involved skin with excoriation and ulceration. Secondary infection may occur. D.D: vulval candidiasis Etiology Local irritants as perfumed soap, deodorant, bubble baths, tight clothing, and urine
The incidence is unknown Treatment avoid local cause oral antihistamine topical corticosteroid
Seborrhoeic dermatitis Occurs in areas of the skin where sebaceous glands are active, such as face, body folds, and less common genitalia The common sites of the vulva are labia majora and mons pubis The lesions are scaly, orange pink in colour and can be secondarily infected Seborrhoeic dermatitis is un common vulval problem Caused by Malassezia infection which is a yeast Treatment: Antifungal as miconazole or ketoconazole cream
Ulcerative dermatomes The ulcerating lesions may be solitary or multiple, painful or non-tender The lesions are uncommon Etiology Herpes simplex virus which are vesicle then ulcerating Syphilis are papule and then ulcerate Chancroid, granuloma inguinale, and lymphgranulma venerum Diagnosis Serology Culture Treatment According to the cause
Genital warts Condylomata accuminata Are caused by HPV. May involve not only the vulval skin but also the vagina and cervix There are more than 50 types of HPV, most important type 6,11,18 Typically lesions are elevated, discrete but sometimes confluent and covering large area Tends to increase in size in patients using COP and during pregnancy The disease transmitted sexually Diagnosis confirmed his pathologically
Treatment Application of 25% tricholacetic acid followed by 25% podophyllin at weekly intervals to lesions and patient asked to bath 6-8h later to remove any excess Podophyllin should not be used during pregnancy If resistant to podophyllin Should be treated by liquid nitrogen application cryosurgery electro diathermy Carbon dioxide laser interferon
Squamous cell hyperplasia This is a diagnosis of exclusion Histologically there is hyperkeratosis, lengthening and distortion of the rete pegs An inflammatory response in the dermis usually occurs, consisting of lymphocytic and plasma cell infiltration The skin is thickened with white hyperkeratosis patches, excoriation and fissures The incidence is unknown but less common than lichen sclerosis
Etiology/risk factors May be the result of repetitive surface irritation and trauma from irritants that cause scratching and rubbing Prognosis The risk of vulval carcinoma has been estimated to be 1-5% Treatment As the lichen scleroses
Benign neoplastic lesions The majority of benign and malignant vulval tumors are of epithelial origin Less commonly they will arise from: epidermal appendages (hid adenoma, sebaceous adenoma) mesoderm (fibroma, lipoma, neurofibroma,leiomyoma, and hemangioma) vestibular glands
Vulval intraepithelial neoplasia Pre-malignant disease of the vulva is much less common than CIN The major factor in the etiology is HPV (type 16, and 33) The incidence varies from 4% if treated to 80% for untreated cases VIN affects mainly labia minora and perineum but may extend to per anal area Presentation pruritus, soreness, and burning in 60% of cases but may be asymptomatic