Download
1 / 24
240 likes | 408 Views
Quality of Life and Depression as Determinants of Treatment Adherence in Hypertensive. Leonelo E. Bautista 1 ; Paul Smith 2 ; Cynthia Colombo 2 ; Dennis G. Fryback 1 ; Lyn Y. Abramson 2 ; Lina M. Vera 1 1 Department of Population Health Sciences 2 Department of Family Medicine. Outline.

E N D
Quality of Life and Depression as Determinants of Treatment Adherence in Hypertensive Leonelo E. Bautista1; Paul Smith2; Cynthia Colombo2; Dennis G. Fryback1; Lyn Y. Abramson2; Lina M. Vera1 1Department of Population Health Sciences 2Department of Family Medicine
Outline Background Objective Study design Data analysis Preliminary Results Conclusions
Background Hypertension affects almost one third of the adults in the US. Being hypertensive increases the chance of developing heart attacks, strokes, heart failure and kidney failure. The chance of developing these diseases decreases significantly if hypertension is detected and treated.
Background Only 53% of known hypertensives receiving pharmacologic treatment have their blood pressure controlled. Almost half of all patients stop taking their antihypertensive drugswithin 12 months after they start treatment. Current adherence-enhancing interventions are complex and labor-intensive and have had little success.
Background • Antihypertensive drugs can have significant positive and negative impact on health related quality of life (QOL) and depression symptoms severity (DSS). • In turn, both QOL and DSS may influence treatment adherence. • There is little or no information on the roles of QOL and DSS on treatment adherence.
Objective To evaluate whether baseline levels and changes in health-related quality of life (QOL) and depression symptoms severity (DSS) are predictive of treatment adherence in newly treated hypertensive patients. Long-term goal: to identify predictors of treatment adherence useful to identify high risk groups and to design effective adherence-enhancing interventions.
Study Design • Longitudinal cohort study among newly identified patients with essential hypertension who require drug therapy. • QOL and DSS (exposure) and treatment adherence (outcome) are evaluated at baseline and at 3, 6, 9, and 12 months after the start of treatment.
Study Design Sample size: 280 newly-diagnosed hypertensive men (n=140) and women (n=140); 21% (n=60) from minority groups Eligibility criteria: 20-69 years old. Not taking mood-modifying drugs This cohort is being recruited and followed at the UW-Department of Family Medicine and WREN Clinics.
Study Design Exposure measurements (QOL and DSS): A short version of the Physical Symptoms Distress Index (PSDI). The Sexual Symptoms Distress Index (SSDI) The Psychological General Well-Being Index (PGWB). The Sleep Dysfunction Scale (SDS). The Beck Depression Inventory-II (BDI-II). Self-administration of the PSDI, SSDI, PGWB and SDS takes about 30-40 minutes.
Study Design Outcome measurements (treatment adherence): Pill count Primary outcome Non-complier: <80% of prescribed pills Self-reported adherence Secondary outcome Blood pressure level Secondary outcome Trained study personnel measure the participant’s blood pressure three times in each visit, with a 2-minute wait between measurements, using an automated device.
Study Design Recruitment: WREN Clinics Hypertensive patients who are about to start or have recently started antihypertensive medication are identified and referred by their physicians or by clinic nurses Study personnel administer screening form to verify eligibility. Eligible patients then are invited to participate.
Study Design Recruitment UW-DFM Clinics Potentially eligible patients are identified through the DFM Clinical Data Warehouse (CDW). A DFM Research Specialist sends a letter to potentially eligible patients informing them about the study and asking whether they may be interested in participating in the study. Informed consent and data collection are conducted at DFM clinics.
Study Desing Follow-up Participants are evaluated at baseline and at 3, 6, 9, and 12 months after the start of treatment. If a participant misses a clinic visit he/she is contacted and invited to come in for a study visit at the DFM or WREN Clinic. Follow-up ends: Participant stops taking his/her medication Drop out Completion of the follow-up period (4th follow-up visit).
Data Analysis Descriptive statistics Survival analysis: Rate of non-adherence in each quarter. Cumulative risk is calculated using the estimated rates (risk=1-exp(-rate*time)) Multivariate analysis Cox regression for cluster data with a robust estimate of the variance to account for the presence of repeated observations.
Preliminary Results Baseline data from 159 subjects Male 59.5% (95%CI: 51.8, 67.2) Average age: 49.1, Range: 23-69 years Follow-up Baseline F1 F2 F3 F4 Total FU 159 114 67 47 29 416 Person time: 807.1 person-months
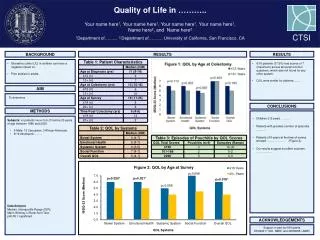
Preliminary Results: Well-being Self-reported health status: Excellent/Very good 60.0% Good 33.5% Fair/Poor 6.5% Psychological General Well-Being Index (PGWB) : Average: 81.2, Range: 19-105
Preliminary Results: Depression Beck Depression Inventory-II (BDI-II) : Minimal (<14) 88.6% Mild (14-19) 5.6% Moderate (20-28) 3.2% Severe (29-63) 2.7% Average 5.4, Range: 0-59 Depression: 11.4% (95%CI: 8.5, 14.8)
Preliminary Results: Compliance _________________________________________________________ Follow- Person- Failures Rate 95% Conf. Cumulative up visit time (100 pm) Interval risk (%) _________________________________________________________ 1 354.0 45 12.7 9.5, 17.0 32.9 2 214.0 11 5.1 2.9, 9.3 14.7 3 146.9 11 7.5 4.2, 13.5 20.9 4 92.2 4 4.3 1.6, 11.6 12.6 Overall 807.1 71 8.8 6.9, 11.0 60.4 _________________________________________________________
Conclusions These are preliminary results. The risk of non-adherence (60% in 12 months) was slightly higher than that reported in other cohort studies. Copayment for medication seemed to improve while an increased number of pills per day seemed to decrease adherence.
Conclusions Better overall quality of life improved adherence. Depression symptoms were not associated to adherence. Age was not associated with adherence.