Download
1 / 1
10 likes | 103 Views
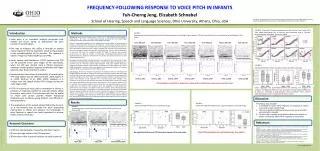
Study explores feasibility of recording Frequency-Following Response (FFR) in infants regarding voice pitch, comparing responses to adults. Detailed methods and data analysis are presented for visualization. Preliminary findings suggest potential to capture FFR in infants as young as one month old. Research questions and key findings are highlighted.

E N D
This study is supported in part by (1) Advancing Academic-Research Career (AARC) Award, American Speech-Language-Hearing Association and (2) Scholarly Activity Award, Ohio University. FIGURE 2 Spectrograms and Autocorrelations from all Infant participants according to age in months. FFR was recordable in the seven infants who participated in this study. Participants: Seven infants (2 males, mean ± SD = 4.14 ± 3.48 months) and nine adults (2 males, mean ± SD = 24.2 ± 2.0 years) were recruited. All infants were from native English speaking households and all adults were native speakers of English. Stimuli: A monosyllabic Mandarin Chinese syllable that mimics an English /i/ was prepared to contrast a rising voice pitch. Stimuli were controlled by a custom-made software written in LabView 8.0 environment. All the tokens were routed through a 16-bit National Instrument PCI 6221 input-output control card with a stimulus sampling rate of 40 kHz. The stimulus signals then routed through a Wavetek low-pass filter (cutoff frequency: 100k Hz, slope 24 dB/octave), an attenuator (TDT PA4) and a headphone buffer (TDT HB6). The stimulus was presented monaurally to the right ear through a custom-built electromagnetically-shielded insert earphone (Etymotics, ER-3A) at a stimulus level of 55 dB SPL. Each session contained two trials of 1200 repetitions each. Recording: Three gold-plated recording electrodes were applied to all participants at the high forehead (non-inverting), right mastoid (inverting), and left mastoid (ground). Recordings were amplified using an electrically isolated, high impedance head stage amplifier (Neuroscan SymAmps2), bandpass filtered at 0.05–3500 Hz (6 dB/octave), and then digitized at a rate of 20000 samples/sec. Continuous data were obtained using Neuroscan Acquire v4.4 software and then stored on a personal computer for offline analysis. Data Analysis:All data was analyzed using MatLab and EEGLab. Continuous recordings were bandpass filtered (100-1500 Hz, 6 dB/oct) and then segmented into epochs of 300 ms in length. A total of 1200 epochs were collected for each condition. An individual epoch was rejected if it contained voltages greater than ±25 µV. During each recording condition, usually less than 100 epochs were rejected in each repetition. The remaining epochs were averaged. Cross correlation of the stimulus and recorded waveforms was performed to identify the location that contains the maximum cross-correlation value between 2-10 ms response window. A 250 ms segment of the recorded waveform was extracted from the originally recorded waveform starting from the maximum cross-correlation value. Two repetitions of 1200 epochs were performed for each condition. Data obtained from each repetition were analyzed separately. To visualize the response in a spectrogram, a periodicity detection short-term autocorrelation algorithm (Boersma, 1993) was carried out on the recording. The latency of the response was defined as the location of the maximum cross-correlation value between 2-10 ms response window. The amplitude of the response was defined as the peak-to-trough amplitude starting from the maximum positive peak to the following negative trough within the 6-12 ms response window in the autocorrelation output. Preliminary data indicates It is feasible to record FFR in response at voice pitch in infants to as early as one month of age. There is a significant difference between the mean of infant and adult pitch strength. Further data is needed to be obtained from more infants to better characterize infant FFR in response to voice pitch. Research Questions FREQUENCY-FOLLOWING RESPONSE TO VOICE PITCH IN INFANTS Fuh-Cherng Jeng, Elizabeth Schnabel School of Hearing, Speech and Language Sciences, Ohio University, Athens, Ohio, USA One Month One Month One Month Four Month Five Month Seven Month Ten Month Infant_001Infant_003 Infant_009 Infant_007 Infant_002 Infant_006 Infant_008 (1) What is the feasibility of recording FFR from infants? (2) How does age relate to the FFR response? (3) How does infant response compare to adult response? Introduction Methods Aiken, S.J., Picton, T.W. (2006). Envelope following responses to natural vowels. Audiology & Neuro-Otology, 11(4), 213-232. Dajani, H.R., Purcell, D., Wong, W., Kunov, H., Picton, T.W. (2005). Recording human evoked potentials that follow the pitch contour of a natural vowel. IEEE Transactions on Biomedical Engineering, 52(9), 1614-1618. Boersma, P. (1993). Accurate short-term analysis of the fundamental frequency and the harmonics-to-noise ratio of a sampled sound. Proceedings of the Institute of Phonetic Sciences, 17, 97-110. Gardi, J., Salamy, A., Mendelson, T. (1979). Scalp-recorded frequency-following responses in neonates. Audiology: Journal of Auditory Communication, 18(6), 494-506 Hu, J., Jeng, F.-C. (2009). An automatic algorithm for detection human frequency following response to voice pitch. In: Abstracts of American Auditory Society Annual Meeting, Poster #31, Scottsdale, Arizona, March 5-7, Krishnan, A., Xu, Y., Gandour, J., Cariani, P. (2004). Human frequency-following response: Representation of pitch contours in Chinese tones. Hearing Research,189,1-12. Krishnan, A., Xu, Y., Gandour, J., Cariani, P. (2005). Encoding of pitch in the human brainstem is sensitive to language experience. Cognitive Brain Research, 25(1), 161-168. FIGURE 1 Typical spectrogram and autocorrelation function of Infant, Adult, and Control FFR. Results Discussion FIGURE 5 Extracted F0 contour comparisons of the stimulus, Trial 1, and Trial 2 from Infant participants. The f0 contours were extracted using a “spectral-density-maxima” algorithm (Hu & Jeng, 2009). FIGURE 6 Comparison between Infant and Adult r values, dc offset, and slope. Linear regression was performed between the stimulus and response f0 contours. No significant difference was observed in the correlation coefficients, dc offset (i.e., intercept), or slope between infants and adults. That is, infant’s pitch-tracking accuracy is comparable to that in adults. Voice pitch is an important auditory perception that reflects the brain’s ability to differentiate the pitch contour of speech signals. One way to measure this ability is through an evoked neural response from the brainstem which is phase locked to the periodicity/pitch of the stimulus. This response is called a Frequency Following Response (FFR). Gardi, Salamy and Mendelson (1979) reported that FFR can be assessed in the early stages of life. Specifically, when the FFR was elicited using a 250-Hz toneburst, neonates showed greater response amplitudes and longer latencies than those recorded in adults. Recent studies have shown the feasibility of recording the FFR using speech sounds (Aiken & Picton, 2006; Dajani et al., 2005; Krishnan et al., 2004, 2005). However, it is unclear how the speech-elicited FFR changes during the early stages of life. If FFR in response to voice pitch is recordable in infants, it provides an objective method to evaluate infant’s ability to process voice pitch. This technique will also be useful for those who cannot provide reliable behavioral feedback, such as infants, young children, and difficult-to-test populations. The implications of the speech-elicited FFR will be to use it as a non-invasive way to study the pitch processing mechanisms in infants and advance our knowledge in what features in speech are most important to achieve better speech perception. References It is feasible to record FFR in response to voice pitch in infants to as early as one month of age. FIGURE 3 Infant and Adult FFR latencies as a function of age. FIGURE 4 Infant and Adult FFR amplitude (i.e., pitch strength) as a function of age. No significant difference in FFR latencies between Infants and adults. Infant FFR amplitudes are significantly larger than adults. Infant_003 Adult_010 Control (Infant_003) Email: jeng@ohio.edu