Download

1 / 15
150 likes | 193 Views
Evaluate US cost-effectiveness over 5 years and lifetime of simvastatin 40mg daily in 20,536 people at varying vascular disease risks. Results show overall effectiveness, cost savings, and suitability for a broad range of individuals. Slides available at www.hpsinfo.org.

E N D
US cost-effectiveness of simvastatin in 20,536 people at different levels of vascular disease risk: randomised placebo-controlled trial • UK Medical Research Council ($14M); British Heart Foundation ($2M); Merck ($8M); Roche Vitamins ($8M) • Designed, conducted & analysed • independently of all sources of support
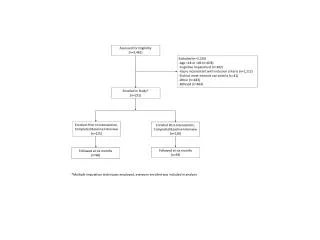
HPS: Eligibility criteria • Increased risk of CHD death due to prior disease • Myocardial infarction or other CHD • Occlusive disease of non-coronary arteries • Diabetes mellitus or treated hypertension • UK adults aged 40-80 years • Total cholesterol 135mg/dl ( 3.5 mmol/l) • Statin or vitamins not considered clearly indicated or contraindicated by patient’s own doctors
Two questions addressed for people at different vascular disease risk • What is the US cost-effectiveness of allocation to simvastatin 40mg daily over the 5-year timescale of the trial? • What is the US cost-effectiveness of simvastatin 40mg daily continued for life?
Vascular disease risk subgroups in HPS Cox model on baseline characteristics used to create five similar sizes multivariate risk groups
Economic analyses using US costs Study simvastatin (40mg at $3.83 daily) & any non-study statin (2003 Wholesale Acquisition Costs) Hospitalisations for vascular events mapped into CMS DRGs; 2003 average Medicare payments Costs and outcomes discounted at 3% per annum
Within trial cost-effectiveness in vascular disease risk subgroups • Analyses in different subgroups indicate: • Similar relative reductions in major vascular events (MVEs) of ~ 25% • Similar relative reductions in costs of vascular event hospitalisations of ~19% • Similar additional statin treatment costs of ~ $5,500 • Hence,UScost effectiveness of statin per MVE and per vascular death avoided was estimated for subgroups by applying overall treatment effects to placebo event rates and costs observed in each subgroup
Methods for lifetime extrapolation model Predicts future non-fatal vascular events, vascular deaths and vascular hospitalisation costs from HPS within trial data Uses US life-table to predict non-vascular deaths Adjusts survival for US age and sex specific quality of life Estimated outcomes: • Life year gained (LY) • Cost per quality adjusted life year gained (QALY)
Within trial validation of the model for major vascular events
Lifetime statin treatment: Life years gained as estimated from the model 5-year major vascular event risk
Lifetime treatment: Cost per Quality Adjusted Life Year gained
CONCLUSIONS: US cost-effectiveness of simvastatin 40mg daily • At current US prices, statin cost-effectiveness is chiefly determined by an individual’s overall risk of vascular events (rather than age or single risk factors, such as LDL) • In the US, statin treatment is cost-effective (i.e. less than $50,000 per QALY) for a wide range of individuals at major vascular event risk as low as 2-3% per annum • At lower prices of generic statins cost-effectiveness of statins would improve
Slides will be available at: www.hpsinfo.org