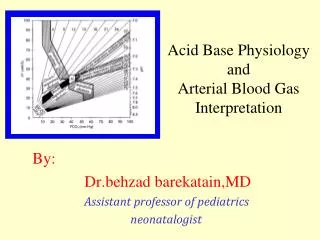
Acid-Base Physiology
Acid-Base Physiology. Terminology. Acidosis - process leading to lower pH Acidemia - low arterial pH (<7.35). Alkalosis - process leading to higher pH Alkalemia - high arterial pH (>7.45). Case #1. 26 YO male involved in MVC Hypotensive and tachycardia at crash scene

Acid-Base Physiology
E N D
Presentation Transcript
Terminology • Acidosis - process leading to lower pH Acidemia - low arterial pH (<7.35). • Alkalosis - process leading to higher pH Alkalemia - high arterial pH (>7.45)
Case #1 • 26 YO male involved in MVC • Hypotensive and tachycardia at crash scene • Altered mental status and multiple severe injuries • pH = 7.38; PaCO2 = 30 mm Hg; HCO3- = 18 mEq/L, Base Deficit = -8 mEq/L Is there an A/B abnormality? What is cause? What other info is needed?
Definitions • Acid: proton (H+) donor HCl↔ H+ + Cl- H2O + CO2↔ H2CO3 ↔ H + + HCO3- • Base/alkali : proton acceptor NH3 + H+↔ NH4 + Strong/Weak acids Strong/Weak bases Physiologically most acids and bases are weak.
Definitions The [H+] of ECF is very low (0.00004 mEq/L = 40 nEq/L). Normal variations are aremarkablysmall 3-5 nEq/L. It is customary to express these very small numbers using the logarithmic pH scale. pH = “power of hydrogen” pH = - log10 [H+] When [H+] = 10-7 mol/L: pH = - log (10-7) = log (1/10-7)= log 107 pH = 7 pH change of 1 = 10X change in [H+]
Importance Of Maintenance Of pH Between 7.38-7.42 • Altered [H+] results in changes in protein structure • Function of excitable tissues • Acidosis: hypoexcitability, CNS depression • Alkalosis: hyperexcitability, tetany • Tertiary structure and function of: • Enzymes • Receptors and ligands • Ion channels • Transporters • Structural proteins
3 Lines Of Defense Against pH Changes: • Buffering • Changes in ventilation • Changes in renal handling of H+ and HCO3-
Buffers Are The1st Line Of Defense. They Minimize (But Do Not Prevent) Changes In pH. • A buffer is any substance that can reversibly bind hydrogen ions Buffer + H+ ↔ HBuffer The effectiveness of a buffer system is measured as buffering power (defined as the number of moles of strong acid added to 1 liter of solution to reduce pH by 1 unit” OR “moles of strong base added to 1 liter of solution to increase pH by 1 unit). “Buffering Power” (β) = Δ[strong acid] / ΔpH
In ECF, the HCO3-/CO2 buffer system is most important: CO2 + H2O ↔ H2CO3 ↔ H+ + HCO3- What Buffer Systems Offer The Most Buffering Power? • Intracellular proteins • HCO3-/CO2 • plasma proteins • inorganic phosphate
Yes, HH predicts plasma pH….. pH = 6.1 + log [HCO3-] / 0.03 x PCO2pH = 6.1 + log (24 / 0.03 x 40)= 7.4 Henderson-Hasselbalch Equation pH = pKa + log(HCO3- / s.PCO2) pKa = 6.1
What Is The Central Message Of Henderson-Hasselbalch? pH = pKa + log(HCO3- / s.PCO2) Plasma pH is a simple function of the HCO3-: PCO2 ratio HCO3-: PCO2 ↑ = pH ↑ (ALKALOSIS) : Could occur due to either HCO3-↑(Metabolic alkalosis) or PCO2 ↓ (respiratory alkalosis) HCO3-: PCO2 ↓= pH ↓( ACIDOSIS) : Could occur either HCO3-↓(metabolic acidosis) or PCO2↑ (respiratory acidosis)
Respiratory System is the Second Line of Defense The second line of defense against acid base changes is control over ECF CO2 concentration by the lungs. Normal pulmonary function balances CO2 excretion with metabolic CO2 production. Increased ventilation decreases ECF [H+] (raises pH), whereas decreased ventilation increases ECF [H+] (lowers pH). These changes occur rapidly through the bicarbonate buffering equilibrium. Not only does the alveolar ventilation rate influence pH by changing PCO2, but the pH in turn affects the rate of ventilation. An acid stimulus is especially effective at increasing the rate of ventilation and CO2 elimination. Recall that the presence of H+ sensors in peripheral chemoreceptors can explain this ventilatory response to the presence of excess metabolic acid. CO2 sensing in both peripheral and central chemoreceptorsshould prevent acidemia resulting from volatile acid (CO2) accumulation, assuming there is normal pulmonary function. CO2 + H2O ↔ H2CO3 ↔ H+ + HCO3- Diagram after A Guyton
The Renal System Is The 3rd Line Of Defense. Changes Are Slow But Powerful 1. Regulation of plasma HCO3- 2. Excretion of fixed (metabolic) acid load • …..Most of the time the urine is acidic to balance metabolic acid production(Acidin the urine is mainly in the form of ammonium ions (NH4+) and phosphoric acid (H2PO4-).
Cellular Respiration Produces CO2 And “Metabolic Acids” ECF Cells Buffering metabolic acid consumes ECF HC0-3 HC03- Food H+ + CO2 CO2 CO2 Lung
H2CO3 H2CO3 CA H2O + H2O + CO2 CO2 Acid Secretion In The Proximal Tubule Recovers Filtered HCO3- Lumen Blood filtration Na+ 3Na+ NHE3 HCO3- H+ 2K+ Na+ NBC 3HCO3- CA CA = carbonic anhydrase Note the net action of this mechanism is reabsorption of Na bicarbonate. NO NET ACID EXCRETION OCCURS.
Acid Is Excreted As Ammonium Ions, Replenishing ECF HC03- lumen blood glutamine NH4+ NH4+ 2HCO3- glutamic acid Na+ NH4+ -ketoglutarate Proximal/distal tubules the net effect of this model is excretion of hydrogen ion(as NH4+), plus generation of new bicarbonate.
Excretion Of “Titratable Acid” Also Generates New HC03- Lumen Blood filtration Na+ 3Na+ NHE3 H+ 2K+ HPO42- Na+ H2CO3 NBC H2O H2PO4- + 3HCO3- CO2 CA Proximal tubule cell
Intercalated cells , A H+ HCO3- ATP K+ Cl- H+ , B ATP Cl- H+ HCO3- In The Collecting Duct H+ Is Secreted Up A Steep Electrochemical Gradient pH=7.4 PT pH=6.8 LOH pH=6.0 DT + CD pH=5.5 to 4.5
ECF Volume and Acid-Base Interactions • ECF volume contraction • ↑ Proximal tubule Na absorption = ↑ HCO3- absorption • RAS activation = ↑ aldosterone = ↑ H+ secretion • Directly (H pump) • Negative luminal potential (Na reabsorption) • hypokalemia • “Contraction alkalosis” – ECV is dominant!
H+ K+ H+ And K+ Interaction In The Renal Collecting Duct Acidosis H+ Hyperkalemia K+ Alkalosis K+ depletion
Summary Of Renal Acid Base Handling • Functions of the renal system in acid base balance • Mechanisms for acid excretion, bicarbonate reabsorption and new bicarbonate generation. • Renal responses to acid base disorders • Interactions between volume and potassium balance and acid-base balance