Download
1 / 48
490 likes | 708 Views
-EURAMA- CREATING PERFECT HEALTH IN EUROPE THROUGH AYURVEDA. Prof. Gerard Bodeker, Dept of Clinical Medicine, Division of Medical Sciences, University of Oxford, Oxford, UK & Dept of Epidemiology, Mailman School of Public Health, Columbia University, New York, USA www.giftsofhealth.org.

E N D
-EURAMA-CREATING PERFECT HEALTH IN EUROPE THROUGH AYURVEDA Prof. Gerard Bodeker, Dept of Clinical Medicine, Division of Medical Sciences, University of Oxford, Oxford, UK & Dept of Epidemiology, Mailman School of Public Health, Columbia University, New York, USA www.giftsofhealth.org
OVERVIEW • PRIORITIES - Identifying EURAMA’S strengths & priorities for the development of Ayurveda in Europe • POLICY – International Policy, EU Policy, EURAMA policy • PRACTICE– Best practice • PARTNERSHIPS – Ayurveda, Modern medicine, Science • POWER – Knowledge is Organizing Power. Generating influence through vision, knowledge, sattva • EDUCATION – orientation, clinical skills development, professional training • EVIDENCE – what evidence exists? what evidence is needed? What evidence can be generated through the EURAMA & the EU in partnership with centres of excellence in India and globally? • EVALUATION – what is the impact of what EURAMA does? Evaluation for advancement
PRIORITIES - EURAMA • An association for doctors and vaidyas • to maintain an academic framework • by creating a platform for scientific research and exchange within the medical profession, • thereby ensuring the public and political acceptance of Ayurveda • as a science and valuable medical practice • for the individual and society
POLICY .
Policy – India & China • INDIA – NATIONAL POLICY In India, formal recognition for Indian systems of medicine came with the Indian Medicine Central Council Act of 1970. In 2002, India developed a specific national policy to facilitate the integration of these health care systems into national health programmes. The policy emphasizes affordability, safety, efficacy and the sustainable use of raw materials (Lavekar & Sharma, 2005). • CHINA - NATIONAL POLICY The Government’s commitment to “develop modern medicine and Traditional Chinese Medicine” has been written into the National Constitution and the two are regarded as of equal importance (Baoyan, 2005).
China – India: differences • Today acupuncture is a licensed practice in most industrialised countries & there are professional bodies, standardised curricula and regulatory boards for acupuncture in these countries. • There are also WHO Guidelines for correct practice of acupuncture & for research into acupuncture. • Similarly, there are WHO standards for safety and evaluation of Chinese herbal medicines.
WHO Support • There are 7 WHO Collaborating Centres on TCM in China and 1 in Australia. • 2 centres in South Korea, 1 in North Korea, 1 in Vietnam, and 2 in Japan are on systems derived from TCM • No WHO Collaborating Centres on Ayurveda or other ISMs
What China has done to promote TCM • For more than a decade, China has had a sub-ministry of Traditional Chinese Medicine (TCM), with ten departments. • These include departments for professional licensure, TCM research, product standards, education etc. • There is an entire department dedicated to foreign trade in TCM.
TCM in the UK • In the UK, every small town can be found to have a Chinese herbalist shop on its High Street. • These are supplied through Chinese Government owned or supported TCM herbal factories & corporations. • Training is provided through Government colleges, including six full national universities dedicated exclusively to training in and research on TCM. • Acupuncture is a licensed profession covered by the NHS • Chinese herbalism will soon be licensed
Africa • Even in Africa, there is an extensive network of TCM practitioners offering services to local Chinese and Western communities and to more affluent Africans. • They import Chinese herbs, which represents foreign exchange earnings for China. Much of this is supported by the Local Chinese Embassy. • There are Chinese Government funded research, education and exchange programmes.
Globalization of Ayurveda • Has been led by private sector. Began with MAV, others have followed • No formal Ayurveda lobby with governments or WHO • Restrictions on Ayurvedic herbs • No formal licensure of Ayurvedic practitioners outside South & SE Asia. • No WHO guidelines on any aspect of Ayurvedic practice or research
Global regulatory status of Ayurveda Result: • No internationally accepted Ayurvedic curriculum • Restrictions on Ayurvedic herbs • No formal licensure of Ayurvedic practitioners outside the sub-continent, • No WHO guidelines on any aspect of Ayurvedic practice or research
Policy on Finance: Who pays for TCAM? • A very high proportion of TCAM expenditure throughout the world is covered by out-of-pocket payments or private health insurance. • Consistent trend in West towards utilization by people with a high disposable income.
EU POLICY on FINANCING • Public health insurance is an important funding mechanism in Europe, with 22 European countries offering full or partial reimbursement for selected TCAM therapies (Burford et al, 2007). • In the United Kingdom in 1995, 40% of GP practices provided access to CAM, with 10% of the cost being met by the National Health Service (Thomas et al, 2001).
US & AUSTRALIAN POLICY on FINANCING • Some American medical insurers confer benefits for limited complementary medical services, primarily through employer-sponsored health plans (Pelletier & Astin, 2002). • In the year 2000, 70% of employee-sponsored programs covered chiropractic; 17% covered acupuncture, 12% covered massage, and the numbers dwindled from there for other CAM services (White House Commission on CAM Policy, 2002). • In Australia, since the introduction of a Medicare rebate for acupuncture in 1984, use of acupuncture by medical practitioners has increased greatly. Medicare reimbursements to doctors for acupuncture rose from $7.7 million to $17.7 million (Easthope et al, 1998).
Japan & Korea: POLICY on FINANCING • Since 1976, the Ministry of Health and Welfare of Japan has approved 147 Kampo formulations, as well as their individual herbal components, to be covered by the national health insurance system. • In the Republic of Korea, national health insurance has covered traditional medicine since 1987.
PRACTICE • Establish standards of Best Practice for Ayurveda in Europe. • Draw on Govt of India & All India Ayurveda Congress standards for clinical practice • Work with medical associations & regulatory agencies to ensure acceptability of standards • Address EU’s wellness concerns as well as medical needs
What is wellness? • Wellness has an emphasis which is quite distinct from the mainstream health sciences focus on illness and pathology. • According to the US National Wellness Institute (NWI), wellness is: “an active process through which people become aware of, and make choices towards, a more successful existence”. • NWI identifies six dimensions of wellness: Social; Occupational; Spiritual; Physical; Emotional; Intellectual. • LOHAS – Lifestyles of Health And Sustainability – is a framework that focuses on “health & Fitness; the environment; personal development; sustainable living; and social justice.”
Medispas • A medical spa is a facility whose medical program is run under the supervision of a licensed healthcare professional, according to The International Medical Spa Association. • Industry wide recognition of the need to focus on wellness - need to shift from a technology-driven industry to one that focuses on wellness and preventive health. • Medical Spa Society: Two things are needed -- a physician on premises actively involved in the patient's care and a level of care that will stand up to conventional scrutiny by accepted standards
EVIDENCE BASE FOR AYURVEDA IN EUROPE • PRIORITY DISEASES (Medical perspective). Diseases for which current conventional treatment regimens are unsatisfactory, e.g. many cancers and chronic debilitating conditions, for which the public are turning to Ayurveda & other branches of CM. • PRIORITY POPULATIONS (Public Health Perspective). Also needing attention are the unmet health needs of ethnic minorities, women, children, the poor, the elderly and those with special medical conditions. • PARTNERSHIPS FOR RESEARCH CAPACITY BUILDING. • Research database development, coordination, dissemination • Partnerships with India’s Golden Triangle Initiative, ICMR, AYUSH • Create WHO Collaborating Centres in Europe for research on Ayurveda • Research funding plan for EU • Student fellowships & research fellowships in Ayurveda
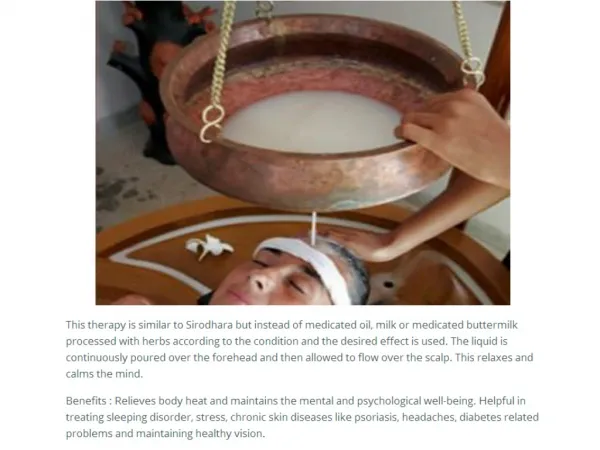
. Evidence base in Asian-themed spas
S Medical Spa, Bangkok • Dr Pakpilai Thavisin, founder director - dermatologist • S Medical Spa is a leading & award winning medical spa in Asia. Offers integrated healthcare service, combining Eastern traditional healing and spa therapies plus the modern Western medical science. • Classic Spa programmes: spa and relaxation, vitality, beauty, figure, holistic, and purification • Three new programmes: • office syndrome: neck, shoulder and back pain as well as headaches due to working at a computer • speedy facial treatment: treatment during lunch break/after work • stress management and sleep medicine: meditationprogram to help people suffering from stress and insomnia
. • The Raj, a New York Times & Conde Naste ‘best destination’ spa, is an Ayurvedic spa in Iowa. • The Raj guests are advised: ‘Lipophilic toxicants (man-made toxins), such as PCBs, DDEs, DDT and other chemicals and pesticides tend to accumulate in our fat tissues. They have been associated with hormone disruption, immune system suppression, reproductive disorders, cancer, and other diseases’ (www.theraj.com)
. • Drawing on published research, clients at The Raj are informed that the Ayurvedic programs offered “are capable of dislodging lipophilic and other toxins from the tissues and reducing their concentration in the body”. • Is this more detail than consumers want? • The Raj has a high percentage of repeat guests.
. .
. ,
. .
. .
EDUCATION • Familiarization • Skills development • Full professional accreditation
CM Education - EU • The German Federal Chamber of Physicians regulates postgraduate CM education of physicians, and CM medical associations have developed an internationally standardised postgraduate education. • In the United Kingdom, Curricula for accreditation of acupuncturists, osteopaths, chiropractors, medical herbalists have been approved. Short courses in CM are offered as part of the undergraduate curriculum in all medical schools, as required by the General Medical Council. • In Hungary, where the practice of therapies such as homeopathy, Ayurveda and traditional Tibetan medicine is restricted to allopathic physicians, these subjects are taught in medical universities.
CM Education - USA • In the United States and Canada, a growing number of universities offer continuing education and elective courses on different CM therapies. • As of 2005, 98 of the 126 medical schools in the U.S. included CAM instruction as part of their required curriculum, as well as a range of TCAM electives (Brixey et al, 2005).
EVALUATION • Build evaluation into all of EURAMA’s activities. • What is the impact of EURAMA’s activities in all of its areas of activity? • What strengths & weaknesses emerge from evaluation? • Set & re-set priorities through evaluation. Evaluate for advancement –
What is needed? • A commitment to support the globalization of Ayurveda in the following ways: • Through development of WHO guidelines on some of the following areas: • curriculum, • clinical practice of Ayurveda, • standards for Ayurvedic herbal preparations, • panchakarma, • yoga instruction, etc.
National & Regional Ayurveda Associations • In partnership with the Govt of India: • Develop/adapt Ayurvedic guidelines and standards, • lobby national EU governments and the EC to strengthen the development of Ayurveda via supportive regulations • Fund & organise conferences that will produce documents, guidelines, curricula etc that can be used nationally, regionally and though the WHO process to establish global standards for a high level of Ayurvedic practice and regulatory support
PRIORITIES • EURAMA’s focus should vary according to national need & regulatory openings. • Adapt EU wide policy goals to national contexts or EC programmes.
Conclusions • Wellness is now a $1trillion industry. The World Bank estimates it to be a $3 trillion industry by mid-century • Within this, Asian healthcare systems & traditions are globalizing • Women are leading the trends. • The Spa industry is the frontline of Ayurvedic expansion in the early 21st Century • Evidence of effectiveness & safety are of key importance to regulators & consumers alike • EURAMA’s time is here. A focus is needed on Policy, Practice, Priorities, Education, Evidence, Evaluation & Power
POWER EURAMA - Generating influence through • vision • knowledge • sattva Knowledge is Organizing Power
. • THANK YOU www.giftsofhealth.org