Download
1 / 25
260 likes | 581 Views
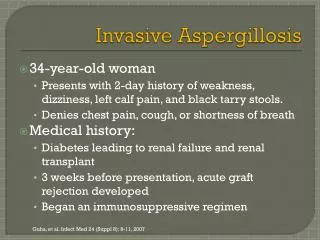
Aspergillosis in CGD. Brahm Segal, MD Roswell Park Cancer Institute brahm.segal@roswellpark.org. Aspergillosis in CGD. Pleural fluid in a CGD patient with invasive aspergillosis. Invasive aspergillosis in a mouse model of chronic granulomatous disease.

E N D
Aspergillosis in CGD Brahm Segal, MD Roswell Park Cancer Institute brahm.segal@roswellpark.org
Invasive aspergillosis in a mouse model of chronic granulomatous disease Segal, BH, N Engl J Med. 2009 Apr 30;360(18):1870-84
Invasive Fungal Infections in CGD • Invasive mould infection is the most important cause of mortality in CGD, with Aspergillus being the most common isolate • 0.1 fungal infections per patient year, despite gamma interferon prophylaxis • X-linked likely at higher risk than autosomal recessive forms Winkelstein et al. Medicine. 2000
Invasive aspergillosis in CGD • Signs of infection in CGD patients may be blunted or non-specific • In a review of aspergillosis in CGD patients at the NIH, one-third of patients were asymptomatic at diagnosis and ~20% had fever • Infection may be detected on routine chest radiographs • Extension to bone may occur • Patients with CGD may have concurrent bacterial and fungal infections • Very important to establish a definite diagnosis Gallin JI et al., Ann Intern Med, 1983; Segal BH et al., Medicine, 1998
Aspergillus and CGD: European experience • Review of 429 European patients with CGD • 67% X-linked • most frequent infections: Staphylococcus aureus (30%), Aspergillus spp. (26%), and Salmonella spp. (16%). • Aspergillus (111 cases) was the most common cause of pneumonia • Bone infection (osteomyelitis) seen in 84 episodes in 56 patients (13%), was caused mostly by Aspergillus spp., followed by Serratia marcescens • Thirty-one patients (7%; 34 episodes) developed a brain abscess, mostly caused by Aspergillus Van den Berg et al, PLoS One 2009;4:e5234
Innate Immunity against Aspergillus Segal, BH, N Engl J Med. 2009 Apr 30;360(18):1870-84
Acute IA ABPA Allergic sinusitis CGD CGD Interaction of Aspergillus with the hostA unique microbial-host interaction Subacute IA CNPA Frequency of aspergillosis Frequency of aspergillosis Aspergilloma Chronic cavitary Chronic fibrosing Immune dysfunction Immune hyperactivity . www.aspergillus.man.ac.uk www.aspergillus.man.ac.uk
Mulch pneumonitis • Acute severe respiratory illness in CGD patients resulting from inhalation of a high level of moulds • Treated with antifungal agents to control the fungal infection • But also with steroids to reduce the excessive inflammation Siddiqui et al. Clin Infect Dis, 2007
Mulch pneumonitis: successful response to antifungal and steroid therapy Siddiqui et al. Clin Infect Dis, 2007
Current therapy for CGD • Prophylaxis • Antibacterial and antifungal prophylaxis • Recombinant gamma interferon • Therapy • Prolonged courses of therapy • White cell transfusions for severe infections may be administered
Itraconazole prophylaxis in CGD • n=39 • randomized, double-blind, placebo-controlled study • Patients 13 years of age or older and all patients weighing at least 50 kg received a single dose of 200 mg of itraconazole per day; those less than 13 years old or weighing less than 50 kg received a single dose of 100 mg per day • One patient (who had not been compliant with the treatment) had a serious fungal infection while receiving itraconazole, compared with seven who had a serious fungal infection while receiving placebo (P=0.10). • Itraconazole was well-tolerated Gallin et al. N Engl J Med. 2003
Voriconazole • Standard of care as therapy for invasive aspergillosis • Substantial experience in patients with hematological cancers and transplant recipients • More limited experience in CGD • Usual maintenance dose in adults: 200 mg or 4 mg per kg of body weight twice daily • Children require higher mg dosing per kg of body weight Walsh TJ et al. Pediatr Infect Dis J. 2002
Posaconazole • Only available orally • Effective as prophylaxis in certain patients with hematological malignancies and stem cell transplant recipients • Evaluated as salvage therapy for several fungal infections, with the most substantial database in aspergillosis • Experience in CGD patients with mould infections difficult to treat other antifungals is limited, but encouraging Segal BH et al., Clin Infed Dis
Gamma interferon • Activates white cells • Reduced frequency of severe bacterial infections in CGD by ~ 65% • Benefit in reducing fungal infections is less clear • administered by injection (subcutaneously), usually 3-times weekly • Generally well-tolerated, can sometimes cause fatigue or mild flu-like symptoms • Used together with antibacterial and antifungal prophylaxis N Engl J Med, 1991; Bemiller LS et al. Blood Cells Mol Dis. 1995
What you can do to prevent aspergillosis and other mould infections in CGD • Prophylaxis with itraconazole or another agent active against Aspergillus • Mould spores are everywhere in the environment, and it’s impossible to eliminate mould exposure entirely • Avoidance of places and activities likely to be associated with high levels of mould exposure • e.g., Gardening, mulching, construction sites, stagnant water
Stem cell transplantation • Can be curative • But, there are substantial risks related to transplantation • Best suited to CGD patients with an HLA-matched sibling donor • Prior aspergillosis is not a contra-indication to stem cell transplantation
Gene therapy • In theory, CGD would be an ideal candidate for gene therapy • Stem cell disorder in which a small proportion of long-lived gene-corrected stem cells might be sufficient to protect against infections • Effective in mouse models of CGD • Main problem has been to maintain a persistent number of gene-corrected circulating white cells • Newer approaches to gene therapy offer hope that these problems can be addressed Ott MG et al. Curr Gene Ther, 2007