Download
1 / 41
410 likes | 489 Views
Learn about angina, its symptoms, causes, and management based on NICE guidelines in primary care cardiac services. Understand the role of coronary arteries and how angina relates to coronary heart disease. Explore statistics, risk factors, angina types, classification, and effects on patients. Get insights on assessing chest pain and diagnosing angina in the context of infection prevention and control.

E N D
Stable Angina: Management according to NICE guidelines Primary Care Cardiac Service
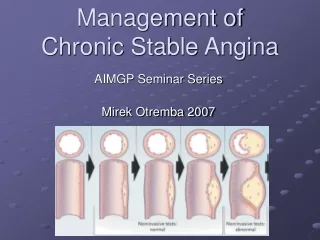
Definition of AnginaBritish Heart Foundation (https://www.bhf.org.uk) • A pain or discomfort most commonly felt in chest, which may also be felt in the arms, neck, stomach or jaw. • Angina occurs when coronary arteries become narrowed and not enough oxygen rich blood can reach the heart muscle, particular when its demands are high, such as during exercise.
Angina is the main symptom of myocardial ischemia and is usually caused by atherosclerotic plaque, obstructing the coronary artery, restricting blood flow, and therefore oxygen delivery to heart muscle. • Provide advice & information about infections & infection prevention & control issues • Write & update infection prevention & control policies that are available on the POD • Provide training & education • Conduct audit
The Coronary Arteries • The coronary arteries supply the heart muscle with blood so that it can pump efficiently • There are two main branches which split to form a network over the surface of the heart • They are about the size of a drinking straw, 2-3mm across • When the heart beats faster, such as during physical exertion or emotional stress, the coronary arteries open up increasing oxygen and nutrient supply to the demanding heart muscle.
The Coronary Arteries in Coronary Heart Disease • The coronary arteries can harden and narrow by the process known as arteriosclerosis. In this process, cholesterol deposits (called plaques) build up in the arterial wall causing the arteries to narrow, restricting blood flow to the heart muscle and causing angina. • There is also a risk that the plaque may break down, causing a blood clot to form. This may block the artery (thrombosis), thereby stopping the blood flow of blood and oxygen to the heart muscle, causing a heart attack (myocardial infarction).
Statistics Statistics Team Number of cases: 71,330 men and 48,405 women in 2014. The population of the UK is 64.1 million. Health survey for England in 2006 reported that 8% of men and 3% of women aged 55-64 years had angina. Figures for ages 65-74 were 14% men and 8% women. • British Heart Foundation (https://www.bhf.org.uk • Guidance.nice.org.uk/cg126 • Provide advice & information about infections & infection prevention & control issues • Write & update infection prevention & control policies that are available on the POD • Provide training & education • Conduct audit
Types of Angina • stable angina – Chronic medical condition where angina attacks are brought on by an obvious trigger (such as exercise) and improve with medication and rest. • unstable angina – where angina attacks are more unpredictable, occurring with no obvious trigger and continuing despite resting.
Risk factors • Smoking • Hypertension • Diabetes • Family history Male <55, Female <65 first degree relative • Raised cholesterol • Overweight • Poor diet • Raised waist measurement • Lack of exercise
Angina classification Canadian cardiovascular society angina classification • Class 1 Ordinary activity such as walking or climbing stairs does not precipitate angina • Class 11 Angina precipitated by emotion, cold weather or meals and by walking upstairs • Class111 Marked limitation of ordinary physical activity • Class 1V Inability to carry out any physical activity without discomfort-angina symptoms, may present at rest • (Campeau L. Grading of angina pectoris. Circulation 1976;1976;54(3):522-23 in sign guidelines)
Effects • A diagnosis of Angina can have a significant impact on patients level of functioning - in one survey angina scored their general health as twice as poor as those who had had a stroke. • A Tayside study showed that patients with angina had high levels of anxiety and depression. (Smith K, Ross D, Connolly E investigating six month health outcomes of patients with angina discharged from chest pain service, European Journal cardiovascular nursing 2002;1(4):253-64 in sign guideline)
Assessing chest pain & Control Team • Location. • Radiation. • Severity. • Duration. • Frequency. • Factors that provoke or relieve. • Provide advice & information about infections & infection prevention & control issues • Write & update infection prevention & control policies that are available on the POD • Provide training & education • Conduct audit
Diagnosis Team • Clinical assessment alone. • Clinical assessment plus diagnosis testing. • Use table of people estimated to have coronary artery disease according to typicality of symptoms, age, sex and risk factors. Remember a significant number of patients with chest pain may not have angina and assessment should try and identify alternative diagnosis at an early stage • Provide advice & information about infections & infection prevention & control issues • Write & update infection prevention & control policies that are available on the POD • Provide training & education • Conduct audit
& Control Team Assessing and diagnosing suspected stable angina (Nice guidelines) • Provide advice & information about infections & infection prevention & control issues • Write & update infection prevention & control policies that are available on the POD • Provide training & education • Conduct audit
Simplified, what Nice says about chest pain diagnosis & Control Team • If patient presents with chest pain or had chest pain in last 12 hours with abnormal ecg or unavailable ecg he should be seen as emergency admission. • If ACS suspected but no pain in last 12 hours and ECG normal refer for urgent same day assessment. • If chest pain more than 72 hours, clinical assessment, ECG , Tropi levels, clinical assess how urgent they should be seen. • Provide advice & information about infections & infection prevention & control issues • Write & update infection prevention & control policies that are available on the POD • Provide training & education • Conduct audit
Making a diagnosis & Control Team • Angina pain is constricting discomfort in chest, neck, shoulders, jaw or arms. • Precipitated by physical exertion. • Relieved with GTN or rest • 3 factors = typical angina • 2 Factors= atypical angina • 1 factor non angina chest pain • Provide advice & information about infections & infection prevention & control issues • Write & update infection prevention & control policies that are available on the POD • Provide training & education • Conduct audit
More factors to consider • Anaemia • Glucose levels • Thyroid function tests • Depression and social isolation
Angina pathway GP diagnosis. Then to either:- • Accident and Emergency • Rapid access chest pain clinic Nottingham City Hospital for further investigations • If likelihood greater than 90% diagnostic investigation not required - manage as angina
In Rapid access chest pain clinic & Control Team • Review risk with table • If risk >90% assume angina. • If estimate risk of CAD 61-90% invasive coronary angiography will be first line diagnostic investigation if appropriate • If risk of CAD 30-60% Non invasive functional imaging will be offered • If risk of CAD10-29% CT scoring will be done CT calcium scoring • 0 =normal >400 offer invasive angiography • Provide advice & information about infections & infection prevention & control issues • Write & update infection prevention & control policies that are available on the POD • Provide training & education • Conduct audit
Investigations • CT scan • Functional imaging • Stress Echo • MRI scan • Invasive angiography
Management Aims & Control Team • To stop or minimise symptoms. • Improve quality of life and long term morbidity and mortality. • Management options include lifestyle advice, drug treatment and revascularisation using percutaneous or surgical techniques. • Provide advice & information about infections & infection prevention & control issues • Write & update infection prevention & control policies that are available on the POD • Provide training & education • Conduct audit
When angina diagnosed Team Management includes • lifestyle advice • drug treatment or revascularisation using percutaneous or surgical techniques or combination • Give the patient the information to safely manage their condition • Provide advice & information about infections & infection prevention & control issues • Write & update infection prevention & control policies that are available on the POD • Provide training & education • Conduct audit
Analysis of comparative efficacy of treatments for people with stable angina • Analysis is difficult because of recent advances in medication and revascularisation strategies over several decades • Trials of drug treatments versus coronary artery bypass surgery in patients were carried out more than 25 years ago and showed a survival advantage with surgery in patients with severe coronary artery bypass surgery, but this was pre statins and other secondary prevention treatments and these treatments have had a significant effect on morbidity and mortality. • Provide advice & information about infections & infection prevention & control issues • Write & update infection prevention & control policies that are available on the POD • Provide training & education • Conduct audit
Nice advises key priorities are to: & Control Team • Explore and address issues according to personal needs. • Self Management skills such as pacing their activities and goal setting, explore impact of stress, advice about physical exertion • Offer optimal drug treatment consisting of 1-2 antianginal drugs as necessary plus drugs for secondary prevention • Revascularisation (CABG) or percutaneous coronary intervention (PCI) for people with stable angina whose symptoms are not satisfactorily controlled with optimal medication • Provide advice & information about infections & infection prevention & control issues • Write & update infection prevention & control policies that are available on the POD • Provide training & education • Conduct audit
Nice recommends & Control Team • GTN spray • Consider Aspirin 75mg taking into account risk of bleeding • Consider ACE • Offer Statin treatment • Offer treatment for hypertension • Offer optimal treatment 1-2 antianginal drugs • Provide advice & information about infections & infection prevention & control issues • Write & update infection prevention & control policies that are available on the POD • Provide training & education • Conduct audit
Drugs for treating Angina as Nice guidelines & Control Team • Beta-blocker or calcium channel blocker first line treatment, with decision based on co morbidities, contraindications and persons preference • If cannot tolerate either of these offer other option • If symptoms not controlled on either consider switching or offering both • Provide advice & information about infections & infection prevention & control issues • Write & update infection prevention & control policies that are available on the POD • Provide training & education • Conduct audit
Drugs for treating Angina & Control Team Nice says If neither beta-blocker or calcium channel blocker not tolerated consider monotherapy of either • Long acting nitrate • Ivabradine • Nicorandil • Ranolazine • Decision based on co morbidities, contraindications and persons preference and cost • Provide advice & information about infections & infection prevention & control issues • Write & update infection prevention & control policies that are available on the POD • Provide training & education • Conduct audit
Nice says consider adding third anti angina only if…. Team • Symptoms are not satisfactorily controlled. • Person awaiting revascularisation or revascularisation is not considered appropriate or acceptable • Provide advice & information about infections & infection prevention & control issues • Write & update infection prevention & control policies that are available on the POD • Provide training & education • Conduct audit
Nice advises people with symptoms not satisfactorily controlled with optimal medication. & Control Team • Will be considered for CABG or PCI. • Angiography will be offered to guide strategy for treatment. • Provide advice & information about infections & infection prevention & control issues • Write & update infection prevention & control policies that are available on the POD • Provide training & education • Conduct audit
Primary care cardiac team: Who are we? • A multi-disciplinary team comprising of: • Community Heart/TIA Nurses • Cardiac Physiotherapists • Occupational Therapist • Assistant Practitioner • Heart Failure Specialist Nurses • Administrator • Volunteer Counsellors • Support from secondary care cardiology
Primary Care Cardiac Service as part of the chest pain pathway Cardiac rehabilitation • ACS • Following Revascularisation • Stable heart failure • STABLE ANGINA • Post valve surgery, heart transplant, LVAD’s • TIA
Who • Newly diagnosed patients can be referred once diagnosis confirmed • Any patients with existing stable angina can also be referred if they have had a recent change in their symptoms
Why • There is overwhelming evidence that comprehensive Cardiac Rehabilitation reduces mortality. • There is emerging evidence that it is also associated with a reduction in morbidity and a reduction in unplanned readmissions. • It improves functional capacity and perceived quality of life and supports early return to work. • It aids the development of self management skills • Secondary prevention forms an integral part of the service
The 7 core components of Cardiac Rehabilitation • Health behaviour change and education • Lifestyle and risk factor management • Psychosocial support • Medical risk factor management • Cardio protective therapies • Long term management • Audit and evaluation
We offer information and support for people with stable angina & Control Team • Explain stable angina and include factors that can provoke angina such as exertion, emotional stress, exposure to cold, eating a heavy meal. Discuss long term management. • Advise to seek help if there is a sudden worsening of condition. • Discuss risks and benefits of treatment. • Assess lifestyle and offer interventions. • Explore individual needs. • Provide advice & information about infections & infection prevention & control issues • Write & update infection prevention & control policies that are available on the POD • Provide training & education • Conduct audit
Cardiac Rehabilitation - pathway • Patients are assessed within 10 working days of referral • They will have a case manager who will work with the patient for a minimum of 3 months. • Patients are assessed at home and can access a range of options to meet their needs • Home based 1-1 support • Group classes – Clifton, Bakersfield, Bells Lane • Referred into many other sources of support
Expected outcomes • Maximise uptake of cardiac rehab by providing a personalised programme delivered at a choice of venues. • Improve physical health and quality of life. • Promote and equip patients to self-manage by encouraging goal setting and building on service users’ knowledge base about their condition. • Reduce hospital admissions • Reduce inequalities and improve access for hard to reach groups • Improve the experience and choice of patients by staff having a close working relationship with local GP’s and a depth of specialist knowledge.
How to refer? • Via Nottingham City Health and Care Point • 0300 300 3333 and select option 5 • Online via https://accesstoservices.citycare.org.uk Referrals cannot be made directly to the service although we are happy to speak to you about the suitability of any referral you wish to make
How to contact us • The service is based at New Brook House Room 29 385 Alfreton Road Radford Nottingham NG7 5LR • Tel: 0115 88 34733
References • Nice chest pain of recent onset march 2010 clinical guideline 95 guidance.nice.org.uk/cg95 • Management of stable angina December 2012 126 guidance.nice.org.uk/cg126 • Nice MI secondary prevention 2013 172 guidance.nice.org.uk/cg172 • Management of stable angina 96 at www.sign.AC.UK • British Heart Foundation (https://www.bhf.org.uk • British National Formulary bnf.org • BACPR Cardiovascular diseases prevention and rehab 2012 • Sign guidelines