Download
1 / 45
450 likes | 539 Views
Drug Therapy of HTN. Dr. Shahrzad Shahidi Nephrologist Associate Professor of Isfahan University of Medical Sciences. The Almighty. Pardons & Grants me heaven Even if I don't know a single letter about Crutz Feld Jacob’s Disease Tsutsugamushi Fever Crigler-Najjar Syndrome

E N D
Drug Therapy of HTN Dr. Shahrzad Shahidi Nephrologist Associate Professor of Isfahan University of Medical Sciences
The Almighty Pardons & Grants me heaven Even if I don't know a single letter about CrutzFeld Jacob’s Disease Tsutsugamushi Fever Crigler-NajjarSyndrome South American equine encephalitis and Many and much more rarer topics BUT …….
The Almighty Will drag me to hell and will not pardon My ignorance of even the minute details of HTN My indifference to apply the current knowledge My negligence in screening for HTN, TOD My despondency about preventing TOD My inadequacy in maintaining my patients as normo-tensive as possible – (This is applicable to all common diseases)
"The Goal is to Get to Goal!” • Measurements & goals should be provided to the patient verbally and in writing at each office visit
HTN What we record as B.P. The Truth is It is only a marker of the bigger problem HTN is a multi-organ systemic disease The Problem is HTN is asymptomatic in 85% of cases
For adequate control of B.P. Do you think we can control most of the patients of hypertension with – One drug Two drugs Three drugs Can’t control In most of the patients of hypertension Two drugs are required for adequate control More so if the initial BP is 20/10 above the goal
Paradigm Shift in HTN Therapy It is not just ↓B.P. TODAY we must strive to • Alter the modifiable risk factors • Keep the SBP < 140 & DBP < 90 • Prevent or halt or reduce TOD – • LVH, CHD, CHF, CVA, CKD, PVD & Retino. • Prevent or control DM (as HTN + DM is hazardous) • Prevent or control Dyslipidemia (Endothelial Dysf.) • Reduce morbidity & mortality • Improve QUALY – Quality Adjusted Life Years
Lifestyle Modification • LSM is the sheet anchor in the management of HTN. • This surely reduces the number of drugs used & their dosage in controlling HTN. • Any drug treatment has value only when coupled with LSM.
Treatment Overview • Pharmacologic treatment • Initial therapy • Combination therapy • What to do when a patient is still not at goal? • Follow-up & monitoring • Cases
Without Compelling Indications With Compelling Indications Drug(s) for the compelling indications Other antihypertensive drugs (diuretics, ACEI, ARB, BB, CCB) Stage 1 HTNThiazide-type diuretics for most. May consider ACEI, ARB, BB, CCB, or combination. Stage 2 HTN2-drug combination for most (usually thiazide-type diuretic &ACEI, or ARB, or BB, or CCB) Not at Goal BP Optimize dosages or add additional drugs until goal BP is achieved.Consider consultation with hypertension specialist. Algorithm for Treatment of Hypertension Lifestyle Modifications Not at Goal BP Initial Drug Choices JNC 7 Express. JAMA. 2003 Sep 10; 290(10):1314
What to choose first? • Initial antihypertensive therapy without compelling indications • JNC 6: Diuretic or a beta-blocker • JNC 7: Thiazide-type diuretics • Most outcome trials base antihypertensive therapy on thiazides JNC 7 Express. JAMA. 2003 Sep 10; 290(10):1314
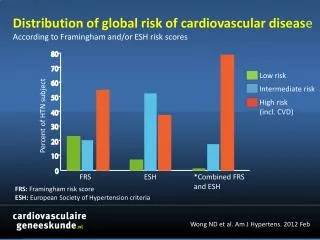
Low Dose Combinations • BP lowering effects from different drug categories were additive 19.9 Law MR et al. BMJ. 2003; 326:1427
Low Dose Combinations • Adverse effects in all drug categories, except ACEI, were dose related • Prevalence of adverse effects in combination was less than additive Conclusion: Utilization of low dose combination therapy can effectively reduce blood pressure while limiting the incidence of side effects Law MR et al. BMJ. 2003; 326:1427
When a Patient is Still Not at Goal? • Optimize dosages or add additional drugs until goal BP is achieved • What do you do when you are using several effective medications? • Consider causes of resistant HTN • Assure drug therapy is rational • “Tricks of the trade”
Identifiable Causes of HTN • Sleep apnea • Drug-induced or related causes • CKD • Primary aldosteronism • Renovascular disease • Chronic steroid therapy & Cushing’s syndrome • Pheochromocytoma • Coarctation of the aorta • Thyroid or parathyroid disease JNC 7 Express. JAMA. 2003 Sep 10; 290(10):1314
Causes of Resistant HTN • Improper BP measurement • Excess sodium intake • Inadequate diuretic therapy • Medication • Inadequate doses • Drug actions and interactions: • NSAIDs, illicit drugs, sympathomimetics, OCP • OTC drugs & herbal supplements • Excess alcohol intake • Identifiable causes of HTN JNC 7 Express. JAMA. 2003 Sep 10; 290(10):1314
Steroids Estrogens NSAIDS Phenylpropanolamines Cyclosporine/tacrolimus Erythropoietin Sibutramine Methylphenidate Ergotamine Ketamine Desflurane Carbamazepine Bromocryptine Metoclopramide Antidepressants Venlafaxine Buspirone Clonidine Drug-Induced HTN: Prescription Medications
COX-2 Inhibitors & NSAIDs • Inhibition of cyclooxygenase, inhibits prostaglandin synthesis that normally maintains afferent arteriole vasodilatation • Afferent vasoconstriction decreases renal perfusion → increased BP • Increasing salt & water retention • Increasing renin release • COX-1 is thought to be primary enzyme responsible for renal vasodilatory prostaglandins
COX-2 Inhibitors & NSAIDs • Case reports of severe increases in BP exists in patients after one dose or more typically after 4 weeks for regular usage • Consider scheduled acetaminophen as an alternative to NSAIDs in patients with difficult to manage HTN Drugs Aging. 2004; 21:479-84; JAMA. 2001; 286:954-59
Drug-Induced HTN: Street Drugs & Herbal Products • Cocaine • Ma huang “herbal ecstasy” • Nicotine • Anabolic steroids • Narcotic withdrawal • Methylphenidate • Phencyclidine • Ketamine • Ergot-containing herbal products • St John’s wort
Food Substances Sodium Chloride Ethanol Licorice Tyramine-containing foods (with MAOI) Chemicals Lead Mercury Thallium & other heavy metals Lithium salts Substances Associated with HTN
Adherence to Medication According to Frequency of Doses Osterberg, L. et al. N Engl J Med 2005
Pharmacologic Sites of Action Veins Heart Arteries
Chinese Menu Approach Veins Heart Arteries • Choose one agent from each category
OK Now what? 2/3 of patients with HTN will need at least 2 medicines for BP control
HTN – Why Combinations ? • If goal BP is not achieved by a single drug in full dose • Then adding another agent will help achieve the goal BP • Two agents sometimes nullify each others side effects • Fixed dose combinations will reduce the no. of tablets • Once daily formulations are good for compliance • Sustained release or LA formulations for 24 h BP control • If three drugs can’t achieve goal BP –Resistant HT
Some Irrational Combinations B blockers + Beta1 stimulants Rebound HT, Paradoxical BP ↑ Beta blockers + Vepapamil Extreme bradycardia, HB, CHF Thiazide + Furesemide Potential volume ↓ and K ↓ CCB + Thiazide No RCTs to support the additive Prazocin + Beta blocker They nullify the effects of each other Verapa/ Dilzem + Nefide No rationale (cardiac actions contridic) Beta blocker + ACEI Not for HT alone, Good for CHF, MI, IHD Sub clinical doses of 2 drugs Try one drug in good dosage, then add 2 drugs of same class No rationale (like Enalapril + Ramipril) (Atenelol + Metoprolol, Nefidepine + Amlo)
Resistant Hypertension • Resistant HT Usually Stage 2 HTN May present in young individuals May have secondary causes • Reasons Not taking medication (liers) Improper BP measurement Excessive Na intake, Inadequate diuretic Rx Full doses of drugs not employed Drug interactions– NSAIDs, SMA, OCP, OTC Herbal remedies, Excessive alcohol use • Rationale Identify the above & correct Secondary causes to be searched for
Follow-up and Monitoring • Patients should return for follow-up and adjustment of medications every 1-2 months until the BP goal is reached • After BP at goal and stable, follow-up visits at 3- to 6-month intervals • More frequent visits for stage 2 HTN or with complicating comorbid conditions • Continue to encourage self BP monitoring • Serum K & Cr monitored 1–2 times per year JNC 7 Express. JAMA. 2003 Sep 10; 290(10):1314
Summary • Lifestyle modifications are important for the prevention of HTN • The goal is to get to goal: • Initial therapy with a thiazide is indicated for most • Consider compelling indications • Initiate low dose combination therapy if BP >20/10 mmHg above goal • Consider the physiologic site of action of agents when choosing combination therapy
Pearls • For resistant HTN – sit down and take a good history • How much water, coffee, milk, juice, tea, ice – anything liquid do you drink daily. • Food preferences & salt intake • Drugs/Alcohol • Compliance
Case 1: Diagnosis AB is a 56 yo female with no significant PMH. Her BMI is 26 kg/m2 and she has a family history positive for Type 2 DM. Her BP measured on 2 consecutive clinic visits is 132/84. What is AB’s BP classification? • Normal • Prehypertensive • Stage 1 Hypertension • Stage 2 Hypertension
Case 1: Therapy What therapy should be initiated for AB? • Enalapril 5 mg PO daily • Hydrochlorothiazide 25 mg PO daily • No therapy is indicated • Lifestyle modifications including weight loss & DASH eating plan should be encouraged
Case 1: Goal of Therapy What is the goal of lifestyle modification in AB? • Goal BP < 140/90, the goal is to get to goal • Goal BP < 130/80, the goal is to get to goal • Improve patients quality of life • Prevent onset of hypertension
Case 1: 5 years later AB, now 59, returns to clinic with marginal success at lifestyle changes. Her BP has repeatedly measured around 146/92. What is AB’s BP classification? • Normal • Prehypertensive • Stage 1 Hypertension • Stage 2 Hypertension
Case 1: 5 years later AB, now 59, returns to clinic with marginal success at lifestyle changes. Her BP has repeatedly measured around 146/92. What should be done? • Enalapril 5 mg PO daily • Hydrochlorothiazide 25 mg PO daily • No therapy is indicated • Reinforce lifestyle modifications including weight loss and the DASH eating plan.
Case 2: Goal of Therapy CD is a 50 yo black male with diet controlled type 2 diabetes. Consecutive BP measurements during recent clinic visits are 162/98 and 158/96. He is diagnosed with Stage 2 Hypertension. What is the goal of therapy for CD? • Goal BP <140/90 • Goal BP <130/80 • Slow the progression of diabetic renal disease by reducing BP to <125/80 • Improve patients quality of life
Case 2: Therapy What therapy should be initiated for CD? • A 6 month trial of lifestyle changes should be initiated immediately • Hydrochlorothiazide 25 mg PO daily • Enalapril 10 mg PO daily • Enalapril / Hydrochlorothiazide 5/12.5 mg PO daily
Case 2: 5 years later CD reaches goal BP of <130/80 after titrating antihypertensive regimen to enalapril/ hydrocholorthiazide 10/25 mg PO QD. At a subsequent follow up visit you learn CD was hospitalized 2 weeks ago for “chest pain”. Reading the discharge summary you note he had ACS for which he was taken to the CATH lab and was found to have 90% occlusion of his LAD which was stented. In clinic his current regimen includes: • Aspirin 81 mg PO daily • Clopidigrel 75 mg PO daily • Enalapril/ hydrochlorothiazide 10/25 mg PO daily