Download
1 / 46
480 likes | 542 Views
Learn how to assess and diagnose spine injuries, common mechanisms of trauma, and imaging modalities. Recognize key fracture types and stability determinants in cervical and thoraco-lumbar spine injuries.

E N D
SPINE TRAUMA CERVICAL SPINE INJURY THORACO-LUMBAR SPINE INJURY
COMMON MECHANISMS OF INJURY HYPERFLEXION- MVA, CAR COMES TO SUDDEN STOP HYPEREXTENSION- MVA, CAR STRUCK FROM BEHIND COMPRESSION- HEAD FIRST DIVE IN SHALLOW WATER
HIGH RISK FACTORS FOR SPINE INJURY HIGH-VELOCITY BLUNT TRAUMA MULTIPLE, SEVERE LONG BONE FRACTURES DIRECT CERVICAL REGION INJURY ALTERED MENTAL STATUS FALL FROM GREATER THAN 10 FEET DROWNING / HEAD FIRST DIVING ACCIDENT SIGNIFICANT HEAD OR FACIAL INJURY NECK PAIN, TENDERNESS, OR DEFORMITY ABNORMAL NEUROLOGICAL EXAMINATION THORACIC OR LUMBAR VERTEBRAL FRACTURE HXISTORY OF PRE-EXISTING VERTEBRAL DISEASE
CLINICAL PROCEDURE INVOLVING PTS WITH SUSPECTED SPINE INJURY PATIENT KEPT IN CERVICAL COLLAR AND IMMOBILIZED ON SPINE BOARD “ABCDEF” ER PROTOCOL FOLLOWED (AIRWAY, BREATHING, CIRCULATION, DISABILITY/DRUGS, EXPOSURE, FOLEY CATHETER) HISTORY AND PHYSICAL (PT HANDLED AS THOUGH SERIOUS INJURY PRESENT) DECIDE IF IMAGING IS NECESSARY
ANT LONGITUDINAL LIG POST LONGITUDINAL LIG LIGAMENTA FLAVA SUPRASPINOUS LIG
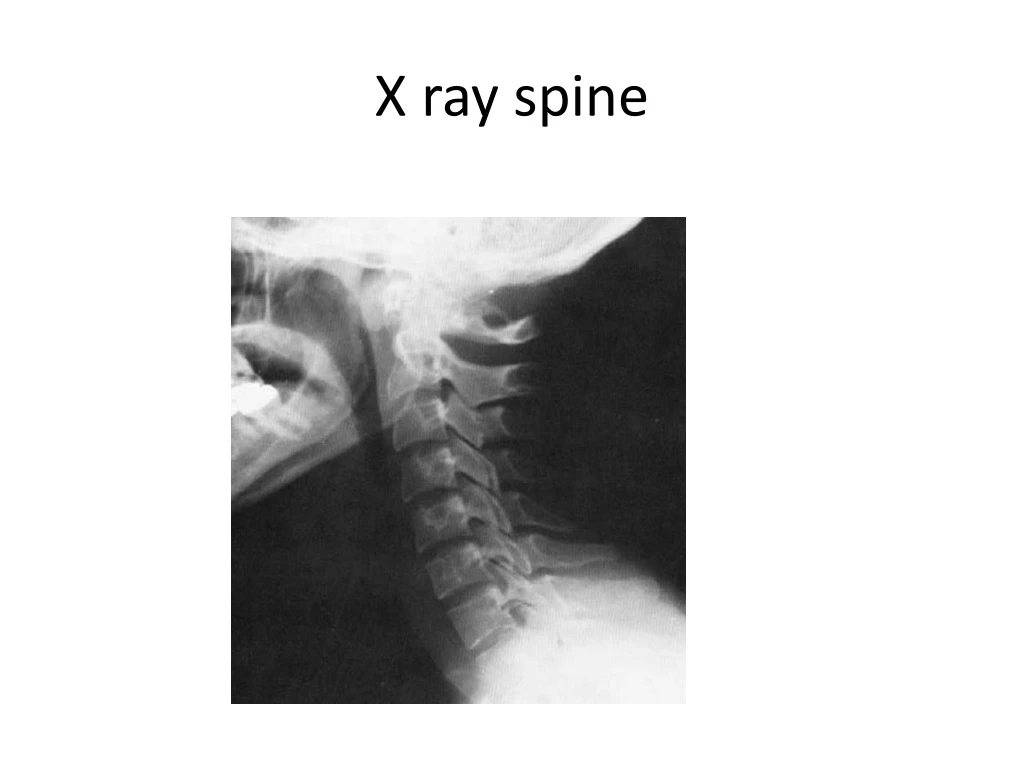
MENU OF IMAGING OPTIONS CERVICAL SPINE PLAIN FILMS ANTERO- POSTERIOR AND LATERAL VIEW STANDARD FIRST LINE IMAGING MODALITY IN ASSESSING CERVICAL VERTEBRAL INJURY SWIMMER’S VIEW
Anteroposterior (A-P) View • Spinous process deviation • Lateral Translation • Coronal deformity
Open Mouth View • Mostly C1-C2 lateral mass • Occipital Condyles/CO-C1 • Odontoid Process
Swimmer’s View • Cervico-thoracic junction • obliques sometimes helpful CASETTE X-ray BEAM
NORMAL C-SPINE VIEWS LATERAL AP ODONTOID
C-SPINE FILM INTERPRETATION 7 STEP PROCESS 1. COUNT VERTEBRAE -C1 THROUGH C7 -IF T1 NOT SEEN SWIMMER’S VIEW 2. ASSESS CURVATURE 3. ASSESS VERTEBRAL ALIGNMENT (4 LINES) -ANT VERTEBRAL LINE -POST VERTEBRAL LINE -SPINOLAMINAL LINE -POST SPINAL LINE 4. ASSESS BONY INTEGRITY 5. ASSESS INTERVERTEBRAL DISK SPACES 6. ASSESS OAA JOINT 7. SOFT TISSUES
THE 4 CONTOUR LINES 1-ANT VERTEBRAL LINE 2-POST VERTEBRAL LINE 3-SPINOLAMINAL LINE 4-POST SPINAL LINE
Lower Cervical Detection • Spinous process gapping • Facet joint Apposition • Inter-vertebral Gapping • Angulation • Translation
Lower Cervical Detection • Spinous process gapping • Facet joint Apposition • Inter-vertebral Gapping • Angulation • Translation
Lower Cervical Detection • Spinous process gapping • Facet joint Apposition • Inter-vertebral Gapping • Angulation • Translation
Lower Cervical Detection • Spinous process gapping • Facet joint Apposition • Inter-vertebral Gapping • Angulation • Translation
Lower Cervical Detection • Spinous process gapping • Facet joint Apposition • Inter-vertebral Gapping • Angulation • Translation
Lower Cervical Detection • Spinous process gapping • Facet joint Apposition • Inter-vertebral Gapping • Angulation • Translation
DENS FRACTURE FRACTURE OF THE BASE OF THE DENS (ODONTOID) OF C2 ANTERIOR OR POSTERIOR DISPLACEMENT OF THE DENS CAN OCCUR AT VARIOUS LEVELS ON THE DENS VIA HYPERFLEXION OR HYPEREXTENSION OF HEAD ON NECK UNSTABLE IF DISPLACEMENT OCCURS
COMPRESSION FRACTURE VARIABLE SEVERITY, FROM MINIMAL ANTERIOR WEDGING TO COMPLETE DISRUPTION OF VERTEBRAL BODY (BURST) LOOK FOR LOSS OF VERTICAL HEIGHT OF VERTEBRAL BODY DUE TO LONG AXIS COMPRESSION OR HYPERFLEXION DIVING INTO SHALLOW POOL STABLE UNSTABLE
TEARDROP FRACTURE AVULSION FRACTURE OF ANTERIOR MARGIN OF VERTEBRAL BODY ANTERIOR LONGITUDINAL LIG INSTABILITY (RUPTURE, AVULSION) HYPEREXTENSION INJURY UNSTABLE INJURY LAMINA MAY JAM TOGETHER CAUSING LIGAMENTA FLAVA TO BUCKLE INWARD AND COMPRESS/CONTUSE THE SPINAL CORD
CLAY SHOVELER’S FRACTURE AVULSION FRACTURE OF SPINOUS PROCESS BY SUPRASPINOUS LIGAMENT USUALLY OCCURRING FROM C6-T2 HYPERFLEXION; DIRECT TRAUMA; DOWNWARD FORCE VIA THORACOSCAPULAR MUSCLE (AS IN SHOVELING MOTION) STABLE
MENU OF IMAGING OPTIONS DORSAL SPINE PLAIN FILMS ANTERO- POSTERIOR AND LATERAL VIEW LUMBO SACCRAL SPINE ANTERO- POSTERIOR AND LATERAL VIEW
Determinants of Stability • T & L spines are more stable than C-spine • Strong ligaments • Stabilization by ribs • Bigger intervertebral discs • Larger facet joints • Less mobility • Fractures & dislocations tend to occur where curvature changes • T11-12 (thoracolumbar junction) • L5-S1 (lumbosacral junction)
Mechanisms of Injury • Hyperflexion +/- rotation • Commonest • Usually see anterior wedge #’s or Chance # • Shearing • Ant or post translation • Hyperextension • Axial loading • Compression or burst #’s
3 Column Model • Anterior column • Ant longitudinal lig • Ant annulus fibrosis • Ant vertebral body • Middle column • Post longitudinal lig • Post annulus fibrosis • Post vertebral body • Posterior column • Spinous processes • Transverse processes • Lamina • Facet joints • Pedicles • Post ligamentous complex • 2 or more columns disrupted = unstable • Most disruption of middle columns are unstable
Stable or Unstable? • Radiographic findings suggestive of instability • Vertebral body collapse w/ widening of pedicles • > 33% canal compromise on CT • > 2.5 mm translation b/w vertebral bodies in any plane • Bilateral facet dislocation • Abnormal widening b/w spinous processes or lamina and > 50% anterior collapse of vertebral body
Stable or Unstable? • Checklist for Instability • Anterior elements disrupted 2 pts • Posterior elements disrupted 2 pts • Saggital plane translation > 2.5 mm 2 pts • Saggital plane rotation > 5o 2 pts • Spinal cord or cauda equina damage 2 pts • Disruption of costovertebral articulations 1 pt • Dangerous loading anticipated 2 pts • 5 or more pts unstable until healed or surgically stabilized
Stable or Unstable? • Risk of neurologic injury increases with • > 35% canal narrowing at T11-12 • > 45% canal narrowing at L1 • > 55% canal narrowing at L2 & below
Approach to T & L Spines • A – adequacy & alignment • All vertebrae need to be visible • Ant & post longitudinal lines • Facet joints should lie on smooth curve • Normal kyphosis & lordosis • All spinous processes should lie in straight line • B – bones • Trace cortical margins of each vertebrae • Difference b/w ant & post body ht < 2 mm • Progressive increase in vertebral body ht moving down spine • Wink sign & interpedicular distance • Don’t forget to look at transverse processes
Approach to T & L Spines • C – cartilage • Progressive increase in disc space moving down spine (except L5-S1) • Facet joint alignment • S –soft tissue • Look at paraspinal stripe and prevertebral space
Injury DetectionThoracic and Lumbar Spines • Same principles • Landmarks and Lines: Lateral View • Posterior VB line • Anterior VB line • Inter-spinous Distance • Translation
Injury DetectionThoracic and Lumbar Spines • Same principles • Landmarks and Lines: A-P View • Spinous process to Pedicles • Inter-pedicular Distance • Translation
Height Loss Adjacent fracture
Transverse process fractures of L2-4 Significance of transverse process fractures is not the fractures in and of themselves but rather the high incidence of associated serious intraabdominal injury (~20%)
Anterolisthesis Of L4 on L5