Nodding Syndrome
390 likes | 453 Views
Learn about the outbreak of Nodding Syndrome in Northern Uganda, its link to onchocerciasis, and key reports from Tanzania, South Sudan, and Uganda. Explore the clinical features, treatments, and ongoing research on this enigmatic disease.

Nodding Syndrome
E N D
Presentation Transcript
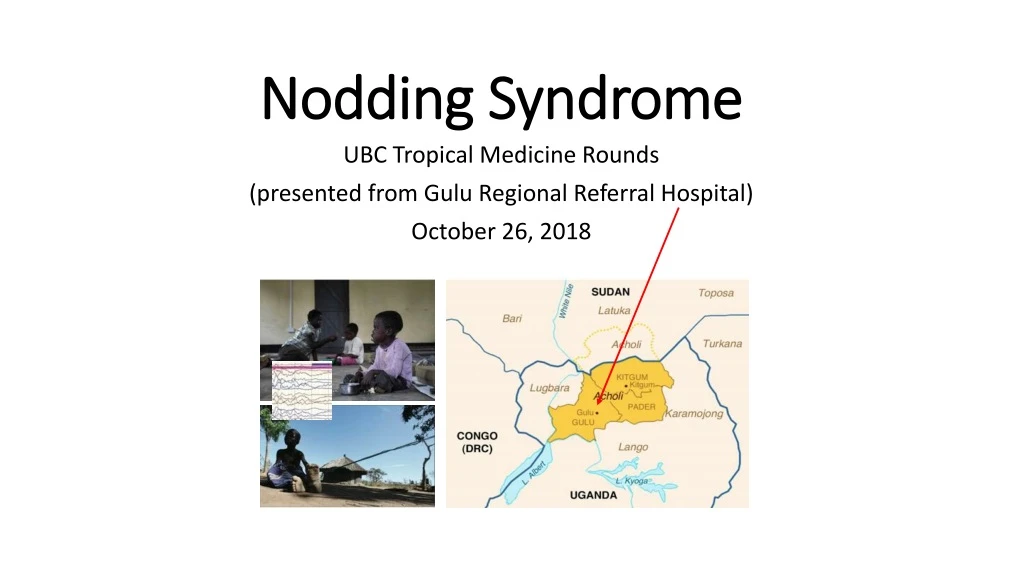
Nodding Syndrome UBC Tropical Medicine Rounds (presented from Gulu Regional Referral Hospital) October 26, 2018
Nodding Syndrome • Outbreak of a mysterious neurological disease among children in Northern Uganda 1997 – 2013 • During a time of humanitarian crises • Form of atonic epilepsy
Nodding SyndromeKey reports • 1965 • Southern Tanzania, Mahenge highlands • Head nodding described as a form of epilespy • Area of poverty and onchocerciasis, Pogorotribe • 2001-2 • South Sudan (WHO) • Area of unrest, internal displacement and onchocerciasis • Survey of the region and case control investigations, with EEG first cases traced back to 1990s • 2009 • Northern Uganda (CDC) • Survey of the region and case control investigation, • Area of humanitarian strife – IDP camps, also onchocerciasis first cases traced back to 2000
Nodding SyndromeTanzania • Dr. Louise Jilek-Aall, • Born in and trained in Norway • Worked as a psychiatrist, Fraser Valley, BC • Taught psychiatry/anthropology at UBC! • Worked in Tanzania in early 60s • Found very high rates of epilepsy • Described nodding as a form of seizures
Cases in TanzaniaMahenge region • Cases were occuring in the community for more than 50 years • Highlands area, Pogoro tribe, poverty and high rates of grand mal seizures • Evaluated 62 patients with Nodding Syndrome • Clinical features, blood, CSF, MRI, EEG • Age onset 5 – 15 years • EEG confirmed interictalepileptic activity in two patients and unspecific changes in four patients. • MRI showed hippocampus pathologies (5/10) and gliotic changes (5/10). • Onchocerciasis • PCR for O. volvulus – positive skin; negative CSF • Skin snip examination for O. volvulus: 61% by microscopy, 84% by PCR • Follow-up about 10 years later • 14/39 cases died • Felt to be a progressive epileptic encephalopathy Epilepsia, 49(12):2008–2015, 2008 African Health Sciences 13(2): 176 – 182, 2013
South Sudan Case control study • 35 cases of Nodding Syndrome evaluated with EEG • 2 – 6% prevalence in some villages (41/1783; 57/854) • Stunted growth; Nodding episodes showed EEG abnormalities • Community believed the condition to be invariably fatal • Link with ochocerciasis (skin snips): 76% case vs. 47% controls (OR] = 3.2)
Nodding Syndromein Uganda • First described in 2000 in Uganda • Peak incidence in around 2001 - 2009 • 3,000 cases of Nodding Syndrome in Northern Uganda • No more cases in the last few years in Uganda • IDP camps closed • Ivermectin MDA programs to eliminate onchocerciasis
GuluNorthern Uganda • LRA (1990s –2006…) • Communities, civilians targetted • > 100,000 people killed • 99% of population in IDP camps • High mortality in the camps • Ebola 2000 • 425 cases, 50% mortality • Nodding syndrome • 3,000 or more cases
Case control studyNorthern Uganda • Associations with: • Onchocerciasis • Exposures to munitions and crushed roots • No associations with: • Urinary thiocyanate concentrations • B6 and deficiencies • Zinc, Mercury, Arsenic, Copper, Lead, Selenium • Measles, HAT, Foltz, PLoS ONE 8: e66419. 2013.
Patients with Nodding Syndrome improve with treatment, Northern Uganda • Follow-up on treatment of 484 patients • Sodium valproate • Supported by village-based lay health volunteers • 40% returned to school • 80% achieved independence in basic self care Idro et al. BMJ Open. 2014 Photo: theinsider.ug
Auto-antibodies to LeiomodinMolecular mimicry with Onchocerca and antibody mediated neurologic dysfunction? • Tested pooled sera of patients and controls with a protein array (>9,000 proteins) • Detected >2 x higher levels of Ab response to 167 proteins • Leiomodin levels were 33,000 x higher • Among individuals, autoantibodies to leiomodin-1 were found in: • 29/55 (53%) of patients with NS • 17/55 (31%) of controls (OR 2.7, 95% CI 1.1 – 6.5). • Anti-leimodin antibodies, were also: • Present in the CSF of patients with NS • Neurotoxic for nerve cell culture • Crossreactedwith Onchocerca tropomyosin (internal muscle proteins) Johnson et al. Sci Transl Med. 2017 Feb 15;9(377)
Auto-antibodies to Leiomodin Johnson et al. Sci Transl Med. 2017 Feb 15;9(377)
Nodding syndrome in Uganda is a tauopathyPollanen et al. • Examined the brains of 5 fatal cases • Northern Uganda • 13 – 18 years at death • Duration of disease 5-10 years • Causes of death • 3 - Malnutrition • 1 - Aspiration • 1 – Lung abscess and empyema • Neurofibrillary tangles were seen preferentially in frontal and temporal regions Acta Neuropathologica Sept 2018
HSV1 encephalitis • 20M, Chinese student • Sudden onset smell disturbance, fear of exercising, fever and headache. Progressed to coma • MRI – temporal lobe changes • EEG – slow waves Gancyclovir and Dexa x 2 weeks
HSV1 encephalitis anti-NMDAR encephalitis • 20M, Chinese student • Sudden onset smell disturbance, fear of exercising, fever and headache. Progressed to coma • MRI – temporal lobe changes • EEG – slow waves Gancyclovir and Dexa x 2 weeks • 3 weeks later • Clinical deterioration again • Abnormal behaviour and movements • NMDAR antibodies detected • EEG – extreme delta brush (EDB) IVIg, Methylprednisone • Improved, but residual memory deficits
HSV1 encephalitis anti-NMDAR encephalitis • Anti-NMDA receptor encephalitis (anti-NMDARE) • associated with psychosis, seizures, dyskinesias, and autonomic instability • Most commonly identified nonviral cause of encephalitis. • Triggers: • NMDAR-expressing ovarian teratoma (<10% of cases) • 20% of HSV1-E have an immune-mediated relapse with anti-NMDARE • Other auto-antibodies are associated with seizure disorders • VGKC Voltage gated potassium channel complex • NMDA N-methyl-D-aspartate • AMPA A-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid • GABA Gamma-aminobutyric acid
Measles and SSPE • Subacute sclerosingpanencephalitis • Chronic and progressive • 1/10,000 cases of measles • 6 – 16 years later • Acute disseminated encephalomyelitis (ADEM) • 1 – 3 weeks after infections • Fever, headache, altered LOC
River blindnessRiver epilepsy? • Seems to be a general association with Onchoceriasis and seizure disorders Colebunders et al. BMC Res Notes (2016) 9:182 Page 8 of 9
Konzo “tied legs” • Epidemicspastic paraparesis • Onset is sudden, symmetrical, affects the legs more than the arms • Permanent disability, but non-progressive course • Severity varies; • Mild just hyperreflexia in the lower limbs • Moderate Standing and walking on the balls of the feet, spasticity and clonus • Severe bedridden - spastic paraparesisand weakness of trunk and arms, impaired eye movements and speech • Occurs in epidemics • War or famine • 1930s first described in DRC > 100,000 cases in DRC • 1980s described in Mozambique • Later also in CAR, Tanzania, Cameroon, Angola • Poverty and food shortages in rural Africa • Predominantly cassava intake Rothe et al. Cases in Clinical Tropical Medicine
Konzo • Cause: • Due to high cyanide + low sulfur amino acid intake • incidence correlated with urinary thiocyanate content • Soaking and then sun-drying cassava flour can remove the cyanide • DDx: • Polio – acute, flacid, asymmetric • TSP (HTLV1) – much more gradual onset
Neurolathyrism • Symmetrical degeneration of pyramidal tracts in the spinal cord, and pyramidal cells in motor cortex • Acute onset, non-progressive • Leg weakness • Caused by: • Consumption of grass peas • β -N oxalyl- L-α, β-diaminopropionic acid (β-ODAP), • An analogue of glutamate • Eating nothing else • Especially and no foods containing sulfur-containing aa’s. Neurobehav ToxicolTeratol. 1983;5:625–9
Food safety • Chemicals in the food itself: • Konzo (cassava cyanide) • Neurolathyrism (grass pea ODAP • Mycotoxins added to the food: • Aflatoxins HCC • Micro-organisms: • Salmonella, Brucella
Association with O. volvulus • But: • Why not in other areas where there is onchocerciasis? • Why also cases in patients without onchocerciasis? • how do the parasites cause brain injury; O. volvulus has never been found in brain tissue or CSF
Onchocerciasis • One of the top 3 human filarial infections • Lymphatic filariasis (LF) • Elephantiasis • Loa loa • Eye-worm • Central and West Africa • Calabar swellings • Complicates treatment reactive encephalopathy • Onchocerciasis: • Spread by black flies • Adult worms live in SQ nodules • Filarial larvae live in the skin and eyes severe itching and blindness
Onchocerciasis • 99% of case occur in Africa • 6 million people infected • Focal disease • Near rivers
Onchocerciasis Clinical features • Blindness • Anterior and posterior segments of eye • Dry, itchy skin • Papular dry and hypopigmented
Onchocerciasis Diagnosis • SIit-lamp exam –filaria, punctate keratitis “snowflakes” • Skin snips • DEC patch test • Serology, molecular
Onchocerciasis Treatment • Ivermectin • Kills the filariae– adult worm can survive for 10 – 15 years • Effect lasts about 6 months – needs to be repeated • Careful in Loa loa endemic areas… • (especially in areas with high prevelance of Loa and low prevalence of Onchocerciasis) • Doxycycline • Kills the endosymbiotic bacteria and, in turn, the adult worm • 200mg OD x 6 weeks – plus ivermectin
Nodding RCT planned Ivermectin in DRC • Patients randomized to start ivermectin • Immediately • After a 4 month delay • Outcome: • Seizures over the next 4 months
Nodding RCT plannedDoxycycline x 6 weeks • Patients randomized to • Doxy 100 daily • Placebo • Follow-up x 24 months • Primary outcome = proportion of Leiomodin antibodies • Functional and neurological assessments also planned
Nodding SyndromeClinical summary • Children • 5 – 15 years, well as infants • Heading Nodding • Triggered by eating, EEG abnormalites • Seizure disorder • Assocoiated cognitive and functional decline, stunted growth, psychiatric illness • Cases clustered in space and time, epidemic like • Time of internal displacement, war, food shortages • Multiple children in same family affected, but not always • Numbers of cases dropped with close of IDP camps • Associated with onchocerciasis infection • Outcomes • Non-progressive in many cases, if treated with anticonvulsants • Deaths from drowning, burns/sepsis
History of Uganda • 1890s – British colony/protectorate • 1962 – Independence • Milton Obote, Idi Amin and Tito Okello were from the north • 1986 • Museveni defeats Tito Okello (who is Acholi) and takes power (NRM party) • Tito OkellofleMembers of the flleeing Ugandan leaders go North • 1987 • IMF – structural adjustment programs • 1987-2006 • LRA • Rebel group, began as a conflict with the military forces of Museveni • the Lord’s Resistance Army (LRA), continues to fight a brutal guerrilla war, in which it claims to be seeking an end to both the marginalisation of the Acholi people and to the Museveni regime • 1994 LRA metamorphosis into a dirty war systemativallyattackingcivilians instead of military targets • Displaced people • 1.8 – 2 million displaced (8% of national population, 94% of regional population) • 250 IDP camps, some housing over 60,000 people • 1,000 excess deaths every week • Higher mortality rate than in Darfur • 95% of residents living in extreme poverty • Abducted children • Over 25,000 children abducted • 80% of the LRA soldieris children • “night commuters” • Eextreme poverty and food insecurity • October 3, 2002 GoU ordered all people in Acholi-Land to move into IDP camps within 48 hour • May 20, 2013: The UN says that the LRA has killed more than 100,000 people over the past 25 years, also blaming it for the abduction of between 60,000 and 100,000 children and the internal displacement of 1.8 million people.
Potential causes : • Toxins • chemicals used during the war • mycotoxins in foods during times of insecurity • Infections • Pattern of an epidemic • EEG ,MRI, and histopath features are not typical of a prion disease • possibly induced by antibodies to O. volvulus cross-reacting with neuron proteins. genetic epilepsy disorders • Nutritional deficiencies • vitamin B6 deficiency was present in the majority of cases (84%) and controls (75%). • Genetic disorder • In about 60% of households more than one child was affected • No genes associated with epilepsy identified