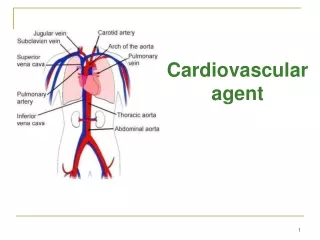
Cardiovascular agent
Learn about antianginal agents like nitrovasodilators and calcium antagonists, their mechanisms of action, side effects, metabolism, and pharmacokinetics. Discover how these drugs treat angina, arrhythmias, and hypertension.

Cardiovascular agent
E N D
Presentation Transcript
Cardiovascular agentThese are drugs used for their action on the heart or other parts of the vascular system. They either modify the total output of the heart or the distribution of blood to the circulatory system.
These drugs are employed in treatment of: 1-Angina 2-Cardiac arrhythmias 3-Hyper lipidemias 4-Disorders of blood coagulation5-Hypertension
Antianginal agent and vasodilators Angina pectoris is characterized by cardiac discomfort caused by inadequate blood supply to the tissue, its main symptom is sever constricting pain in the chest, to the left shoulder and down the arm.
Nitrovasodilators: ♦How do nitrovasodilators work? ♦ What are the unwanted side effects and problems? e.
♦ Metabolised to NO activate guanylate cyclase increase in cGMP fall in intracellular free calcium vascular relaxation increase in venous capacitance fall in central venous pressure reduce preload reduction in ventricular dimensions and cardiac output ♦ Side effect – headache due to dilatation of intracranial arteries Also problem with quickly developing tolerance that can lead to abnormal constriction of coronary arteries following withdrawal
Also antianginal may act by reducing the work done by the heart so the oxygen demand is reduced.
Onset (min) Duration of Action (min) Metabolites Amyl nitrite 0.25 1 Nitroglycerin 2 30 3 60 Active Isosorbide dinitrate Erythrityl tetranitrate 15 180 Pentaerythritol tetranitrate 20 330 Pharmacokinetics of Nitrate Esters • Nitrate esters act fast! Think about the size of these molecules. • They are rapidly metabolized in the liver (glutathione-nitrate reductase). Number of nitrate groups does not linearly correspond to potency • Nitrate esters and possibility of explosion! • Nitrovasodilators decrease the blood pressure of patients!!
Calcium antagonists: Stimulation of the cardiac cell initiates the process of excitation which has been related to ion fluxes through the cell membrane. Ca+2 play an important role in the regulation of many cellular processes. The entry of Ca+2 into the cytosol of the myocardial cells and the release of Ca+2 from intracellular storage sites are important for initiating contraction of the myocardium.
Chemical Type Chemical Names Brand Names Phenylalkylamines verapamil Calan, Calna SR, Isoptin SR, Verelan Benzothiazepines diltiazem Cardizem CD, Dilacor XR 1,4-Dihydropyridines Nifedipine nicardipine isradipine felodipine amlodipine Adalat CC, Procardia XL Cardene DynaCirc Plendil Norvasc Three Classes of CCBs
Verapamil(Isoptin) Verapamil is a phenyl alkylamine Ca+2 channel antagonist. It binds to a specific site on the Ca+2 channels promoting antagonism. This effect result in vasodilatation, so verapamil is used in treatment of angina pectoris, arrhythmias and hypertension
Diltiazem Hydrochloride: Diltiazem undergoes several biotransformation, including deacetylation, oxidative O-demethylation and N- demethylation and conjugation of the phenolic metabolites.
Nifedipine:(Adalate) It is a 1,4-dihydopyridine derivative The nitro group is essential for its antianginal effect, but it is not a nitrate. It has potent peripheral vasodilator properties through the inhibition of Ca+2 channels in the vascular smooth muscle. nifedipine is more effective in patients whose anginal episodes are due to coronary vasospasm ,(why) also it is used to treat hypertension .
The metabolism of nifedipine: 1- Aromatization 2- Hydrolysis 3- Benzylic oxidation 4- Lactonization
Antiarrythmic Drugs: Cardiac arrhythmias are caused by disturbance in the conduction of the impulse through the myocardial tissue or disorders of impulse formation or both.
Quinidine sulphate USP;- ProcainamideHydrochloride USP: (pronestyl) N-(2-Diethylaminoethyl)p-aminobenzamide It acts in a similar way to quindine but it bounds minimally to plasma protein and the plasma level appears 20-30 minutes after administration. Metabolism of procainamide occurs through the action of N-acetyl transferase and about 50 % of it is excreted unchanged. Synthesis of procainamide: An alkaloid obtained from cinchona bark, it is the dextro diastereoisomer of quinine. Quindin reduces the Na+ current by binding the open ion channels, which decrease the conduction velocity.
Lidocaine hydrochloride USP: (xylocaine) It is used as local anesthetic and the drug of choice for parenteral treatment of arrhythmias. It is effective for preventing and terminating ventricular arrhythmias. Lidocaine act by blocking the Na+ channels so causing a slowing down of the conduction time of the impulse through the heart.
Antihypertensive Agents Drugs used to treat Hypertension 1- Ca+ channel blocker 2- Angiotensin Antagonists - Angiotensin-Converting Enzyme Inhibitors (ACE inhibitors) 3- Sympatholytics (SYMPATHETIC DEPRESSANTS 4- Direct - Acting Arteriolar Vasodilators 5- Diuretics
ACE cleaves two amino acids from its substrate to produce Ag-II. As a result, ACE is termed a "dipeptidyl" carboxypeptidase (i.e) it cleaves 2 amino acids.
By preventing the formation of Ag-II, ACE-I also cause a decrease in the production of aldosterone which produces hyperkalemia. ACE-I also inhibits degradation of bradykinin. This causes an elevation of bradykinins which is thought to be responsible for persistent dry cough and angioedema associated with ACE-I. About 10% of the patients using an ACE-I have dry cough. Angiotensin II is generated by two pathways: 1) rennin angiotensin system, and 2) chymases.
Schematic Model of Active Sites of Angiotensin Converting Enzyme
The three classes of marketed ACE-I include: • captopril analogs • enalapril analogs • phosphorous containing analogs. • They all have functional features that allow them to bind to the cationic binding site and the zinc binding site of ACE. The two interactions by ion-ion binding are essential for activity.
Captopril Analogs The pharmacophore is 2D-methyl, 3-mercapto propanoyl-L-proline .This designates a structure with a propanoyl (3 carbon structure with a keto group at the –C1 position) attached to the proline at the amino terminal with the -C1 carbonyl and has a mercapto group at the –C 3 of the propanoyl. Further, the –C2 of the propanoyl has a methyl group. The carboxylic terminal of proline is essential for binding to the cationic site while the mercapto group is essential for binding to the zinc binding site.
Enalapril Analogs The pharmacophore is N-carboxymethyl-L-alanyl-L-proline .It has alanine and proline attached together by an amide bond. At the N-terminal of alanine, there is a methyl with a carboxylic group attached to it. the carboxylic terminal of proline is essential for binding to the cationic site while the second carboxylic group in the free form is essential for binding to the zinc binding site. Phenyl ethyl group in the S-configuration produced the best activity.
Enalpril maleate: (vasotec) It is a long action ACE inhibitor. It requires activation by hydrolysis of its ethyl ester. It has no side effects as those of captopril. Benazepril, Quinapril, Ramipril.
Phosphorous containing Analogs Fosinopril (Fovas) As with the captopril analogs, the carboxylic terminal of proline is essential for binding to the cationic site while the ionized –OH of the phosphinyl group is essential for binding to the zinc binding site.
Angiotensin II Receptor Blockers (ARB) The majority are analogs of the general pharmacophore above: 1-N-benzyl 2-butyl Imidazole Imidazole ring is required to mimic the His6 side chain of Ag-II.
Losartan, Irbesartan, and Candesartan Cilexetil are a nonpeptide antagonist/blocker of one of the angiotensin receptors, the AT1 receptor, resulting in decreased presser effect.
Losartan is an analog of the general pharmacophore (1-N-benzyl 2-butyl Imidazole. The imidazole ring allows for better binding to Ag-II receptor (AT1). The phenyltetrazole acidic group contributes to binding to Ag-II receptor especially with the tetrazole being in the ortho position. Also, the tetrazole group increases metabolic stability, lipophilicity and oral bioavailability. Since there is no linker between the two phenyls, it has good oral activity. The 2-butyl group maintains activity. The methyl alcohol on the imidazole ring is also good for activity.
The parent structure is active but has a short half life (1.5-2.5 hr). The parent structure is oxidized to an active 5-carboxylic acid metabolite which is 10-40 times more potent than parent structure and has a longer half life (6-9 hr). This increases the duration of action and provides for once or twice a day dosing.
Some marketed products do not have (imidazole) it and other five membered heteroaromatic rings including pyrazole and pyrrole ring are acceptable. Also, one product, Valsartan has an open ring imidazole with a keto group that may serve to H-bind to the receptor.
Anti hyperlipidemic agents Hyperlipidemia is the most prevalent indicator for susceptibility to atherosclerotic elevated plasma levels of lipids that are usually in the form of lipoproteins. Lipoproteins are macromolecules consisting of lipid substances (cholesterol, triglycerides) none covalently bound with protein and carbohydrate. The various lipoproteins found in plasma can be 1-Very low density lipoprotein (VLDL) 2-Intermediate density lipoprotein (IDL) 3-Low density lipoprotein ( LDL) 4-High density lipoprotein ( HDL) 5-Chylomicrons
Classification of Antihyperlipidemic Drugs Several different classes of drugs are used to treat hyperlipidemia. These classes differ not only in their mechanism of action but also in the type of lipid reduction and the magnitudeof the reduction.
Drugs for hypercholesterolemia • Bile acid-binding resin • 3-hydroxy-3- methyglutaryl Co A (HMG-CoA) reductase inhibitor • Ezetimibe • Drugs for reducing elevated TG and to raise HDL-C levels • Fibric acid derivatives • niacin
cholestyramine (Questran) • is a non-absorbed bile acid sequestrant that is used a therapy of hyperlipidemia and for the pruritus of chronic liver disease and biliary obstruction. • is a large, highly positively charged anion exchange resin that binds to negatively charged anions such as bile acids • The binding of bile acids to cholestyramine creates an insoluble compound that cannot be reabsorbed and is thus excreted in the feces.
Adverse effects • Beceause they are not orally absorbed, they produce minimal systemic side effects • Constipation • Heartburn, nausea, belching, bloating • These adverse effects tend to disappear over time
Target: HMG-CoA Reductase (HMGR) • The enzyme that catalyzes the conversion of HMG-CoA to mevanolate. • This reaction is the rate-determining step in the synthetic pathway of cholesterole. 3-hydroxy-3-methylglutaryl-coenzyme A (HMG-CoA)
In 1976…….. • metabolites isolated from a fungus (Penicilliumcitrinum) were found to reduce serum cholesterol levels in rats. • This work was done by Akira Endo, Masao Kuroda and Yoshio Tsujita at the Fermentation Research Laboratories, Tokyo, Japan. Today, there are two classes of statins: Natural Statins: Lovastatin(mevacor), Compactin, Pravastatin (pravachol), Simvastatin (Zocor). Synthetic Statins: Atorvastatin (Lipitor), Fluvastatin (Lescol). Statins are competitive inhibitors of HMG-CoA reductase. They are bulky and “stuck” in the active site. This prevents the enzyme from binding with its substrate, HMG-CoA.
SAR of HMG-CoAreductase inhibitors • The structure should contains • lactone ring (sensitive to stereochemistry of it, ability of ring to hydrolyzed, length of bridge) • Bicyclic rings ( could be replaced with other lipophlic rings, size and shape of it are important for activity) • Ethylene bridge between them
Fibrates They are classified as analogues of isobutyric acid derivatives (essential for activity)
SAR of Fabric acid derivatives • They are classified as analogues of isobutyric acid derivatives (essential for activity) Fabric acid
Fibrates are 2-phenoxy-2-methyl propanoic acid derivatives [aromatic ring]-O-[spacer group]-C(CH3)2-CO-OH