Download
1 / 45
450 likes | 667 Views
OSTEOPOROSIS. Information from the 2007–08 NHS suggests that almost 700,000 Australians (3%) have been diagnosed with osteoporosis. Most of these cases occur after the age of 55, and 82% of those reporting a diagnosis of the condition are females.

E N D
Information from the 2007–08 NHS suggests that almost 700,000 Australians (3%) have been diagnosed with osteoporosis. Most of these cases occur after the age of 55, and 82% of those reporting a diagnosis of the condition are females. • However, because osteoporosis has no symptoms, it is often not diagnosed until a fracture occurs. • Data about diagnosed cases are believed to underestimate the actual prevalence of the condition.
The risk of death increases after most types of osteoporotic fractures, but particularly hip fractures. There were more than 1,400 deaths in 2007 where hip fracture was recorded as an associated cause of death. • Osteoporosis was managed at 1 per 100 encounters in 2007–08, equating to around 1 million Medicare-paid GP consultations.
It is estimated that every day 40 Australians break their hips following minimal trauma (AIHW 2010b). • These fractures are a substantial burden on society and the health system, and considerable resources have been dedicated to reducing this burden through raising awareness of the risks for fractures and subsidising services for diagnosing and managing osteoporosis.
The incidence of minimal-trauma hip facture in Australia is declining, with the age-adjusted rates for males falling by 14% and for females by 20% between 1997–98 and 2006–07. • This trend may help offset the expected increase in the absolute number of hip fractures resulting from population ageing over time.
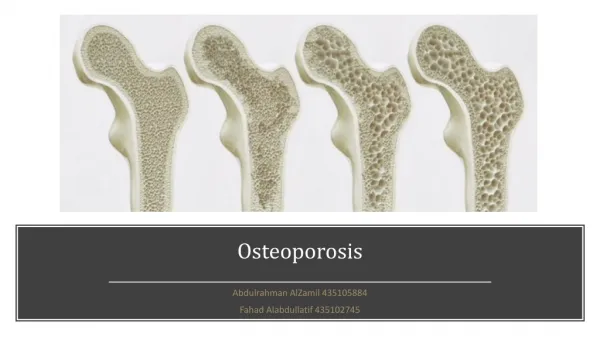
What is osteoporosis?http://www.osteoporosis.org.au/osteo_osteoporosis.php • Osteoporosis is a condition in which the bones become fragile and brittle, leading to a higher risk of fractures (breaks or cracks) than in normal bone. • Osteoporosis occurs when bones lose minerals, such as calcium, more quickly than the body can replace them, leading to a loss of bone thickness (bone mass or density). As a result, bones become thinner and less dense, so that even a minor bump or accident can cause serious fractures. These are known as fragility or minimal trauma fractures.
Any bone can be affected by osteoporosis, but the most common sites are bones in the hip, spine, wrist, ribs, pelvis and upper arm. Osteoporosis usually has no signs or symptoms until a fracture happens - this is why osteoporosis is often called the 'silent disease'. • Every 8 minutes, someone is admitted to an Australian hospital with an osteoporotic fracture. This is expected to rise to every 3 - 4 minutes by the year 2021, as the population ages and the number of osteoporotic fractures increase.
Fractures due to osteoporosis (osteoporotic fractures) can lead to changes in posture (eg developing a stoop or Dowager's hump in your back), muscle weakness, loss of height and bone deformity of the spine. Fractures can lead to chronic pain, disability, loss of independence and even premature death. • Did you know a woman's chances of suffering from an osteoporosis related fracture is greater than her risk of cervical, uterine and breast cancer combined?"
The fracture cascade • 1 in 2 women and 1 in 3 men over 60 years will have an osteoporotic fracture in Australia. • About 50% of people with one fracture due to osteoporosis will have another, and the risk of new fractures rises exponentially with each new fracture the 'cascade effect'. • The 'cascade effect' means that women who have suffered a fracture in their spine are over 4 times more likely to have another fracture within the next year, compared to women who have never had an osteoporotic fracture.
People who have had two or more osteoporotic fractures are up to 9 times more likely to have another fracture, rising to an 11 times greater risk for people who have had three or more fractures, compared to someone who has not had one. • Two thirds of fractures of the spine are not identified or treated, even though they nearly all cause pain and some disability. Often people believe that the symptoms of spine fracture back pain, height loss or rounding of the spine are just due to 'old age'. However, for many people, osteoporotic fractures can be prevented, or at least the risk of having further fractures greatly reduced.
To stop the fracture cascade, it is essential that osteoporotic fractures are identified and treated as quickly as possible.
Osteoporosis in men • With the prolongation of life expectancy, osteoporosis has become an increasing problem in the majority of developed countries worldwide. Every third hip fracture occurs in men, and more than 11% of the male population over the age of 50 years suffer the fracture. • Diagnostic tests for idiopathic osteoporosis are performed in men under 60 years of age without other potential risk factors of developing the disease. In the majority of cases, their low bone mineral density (BMD) is caused by a low peak bone mass.
Secondary osteoporosis occurs in about 30 % of men, and involutionary osteoporosis developed in men over 60 years of age results from their decreased testosterone and IGF-1 levels. • The study results showing that BMD levels in both sexes provide similar fracture risk information suggest that the existing diagnostic criteria for female osteoporosis can also be employed in men.
It has been proved that biphosphonate and teriparitide therapy significantly increase BMD levels in men. The administration of androgens has been shown to be effective in men with hypogonadism, although their validity for patients with eugonadism has not yet been discussed. • An improved knowledge of the bone metabolism and bone remodelling has recently opened the door to an extensive series of molecules that may play a key role in the treatment of male osteoporosis in the future. Kastalan,D. 2007, `Osteoporosis in men’,Arh Hig Rada Toksikol, vol.58, no.1, pp.25-32
Although osteoporotic fractures are less common in men than in women, when they occur, these fractures are associated with higher disability and death than in women. (Osteoporosis Australia)
THE RELATIONSHIP BETWEEN PROTEIN INTAKE AND BONE LOSS (Whitney et al 2011 PP.187-8) • When protein intake is high, calcium excretion increases. However – bones need both protein and calcium. • For most women in Australia, average calcium intakes are lower and protein intakes are higher, yielding a 9 to 1 ratio calcium losses significant enough to compromise bone health. In other words, the problem really is too little calcium not too much protein.
Inadequate intakes of protein may also compromise bone health: • Osteoporosis is particularly common in elderly women and in adolescents with anorexia nervosa – groups who typically receive less protein than they need. • For these people actually increasing their protein intake may be the best way of protecting their bones.
QUALITY OF LIFE ISSUES • The reduced quality of life for those with osteoporosis is enormous. • Osteoporosis can result in disfigurement, lowered self-esteem, reduction or loss of mobility, and decreased independence. • As the disease progresses, osteoporosis sufferers often lose several centimetres in height, 10-15 cm. is not unusual, because the vertebrae in their spine begin to collapse.
Kyphosis can occur in advanced Osteoporosis. Bone becomes so porous that it weakens and fractures spontaneously or with very little pressure. The fractured edge compresses and the vertebrae above it are shifted forward so that the spine is no longer straight upright. It tips forward and Kyphosis or 'dowagers hump' results. If additional vertebrae fracture or crumble, the back hump can become more pronounced. • Many break their hip, and a startling 15% of those who suffer this common osteoporotic injury die as a result of complications such as pneumonia, other infections and cardiac insufficiency.
Researchers in Australia have uncovered what they think is one reason hip fractures are more common in Western countries than in developing countries. • Because children in Western countries have higher than average nutrient intakes than those in developing countries, they grow faster and to a greater extent. • As a result, the part of the thighbone that fits into the pelvis becomes quite long.
The greater the length of this part, called the hip axial length, the more fragile this region of the hip is, and in turn the higher the risk for hip fractures, especially as bone mass decreases with advanced age. • This suggests that people in Western countries especially must pursue strategies to avert hip fracture, notable in later years.
Modifiable Risk factors • Women with anorexia, Celiac disease, diabetes, chronic diarrhoea, kidney, or liver disease are all more likely to develop osteoporosis. • Anorexia Nervosa represents an important risk factor for Osteoporosis. The data in Anorexia Nervosa patients document some statistically significant differences in term of Bone Mass Density, osteoclasia and T-score reduction. (Coaccioli,S. et al. 2007, `Osteoporosis and anorexia nervosa: ultrasonometric and biochemical evaluation--preliminary data’, La Clinica Terapeutica, vol.158, no.1, pp.17-20)
↓Physical activity, ↓calcium intake, ↑coffee, ↑alcohol and ↑tobacco consumption can influence Osteoporosis risk. These factors can be modifiable and, in some cases, their control may contribute for the OP prevention. • Low bone mass in the skeleton, which increases the risk of osteoporotic fracture, also may be associated with periodontal bone loss and tooth loss. Osteoporosis and periodontal disease share several common risk factors, including older age, smoking and perhaps insufficient dietary intakes of calcium and vitamin D. (Kaye,EK. 2007, `Bone health and oral health’, Journal of the American Dental Association, vol.138, iss.5, pp.616-9)
The use of systemic corticosteroids is one of independent risk factors with bone mineral density (BMD) for fractures. The prior and current exposure to corticosteroids confers an increased risk of fracture that is of substantial importance beyond that explained by the decrease of BMD. (Soen,S. 2007 `Secondary osteoporosis. Glucocorticoid-induced osteoporosis: Threshold of bone mineral density for vertebral fracture’, Clinical Calcium, vol.17, no.3, pp.399-402)
There is growing evidence of the existence of a correlation between cardiovascular disease and osteoporosis, irrespective of age. The morbidity and mortality of osteoporosis is mainly related to the occurrence of fractures. • The correlation between osteoporosis and atherosclerosis is being established by studies of the underlying physiopathological mechanisms, which seem to coincide in many biochemical pathways, and of the risk factors for vascular disease, which have also been associated with a higher incidence of low-bone mineral density.
In addition, there is evidence indicating an action of antiresorptive drugs on the reduction of cardiovascular risks and the effect of statins, antihypertensives and insulin on bone mass increase. • The mechanism of arterial calcification resembles the process of osteogenesis, involving various cells, proteins and cytokines that lead to tissue mineralization. Danilevicius,CF., Lopes,JB., Pereira,RM. 2007, `Bone metabolism and vascular calcification’, Brazilian Journal of Medical and Biological Research, vol.40, no.4, pp.435-42
Estrogens also play a role in both CVD and OP through their effects on cytokines, such as IL-1, IL-6 and TNF-alpha and osteoprotegerin (OPG). The lack of estrogens induces an increase in these cytokines and a decrease in OPG, both implicated in the mechanisms of bone loss and atherogenesis. • An additional link between CVD and OP seems to be related to the action of some drugs, such as bisphosphonates, statins and raloxifene. Baldini,V et al. 2005, `Cardiovascular disease and osteoporosis’, Journal of Endocrinological research, vol.28, suppl.10, pp.69-72
There is a relationship between cortisol levels and bone mineral density (BMD) among premenopausal women with major depression. As such, depression should be considered among risk factors for osteoporosis in premenopausal women. (Altindaq,O et al, 2007, `Relation of cortisol levels and bone mineral density among premenopausal women with major depression’, International Journal of clinical practice, vol.61, no.3, pp.416-20) • Osteopenia and osteoporosis are commonly found in IBD patients. Steroid treatment and bowel resection were significant risk factors for osteoporosis of the lumbar spine. However, disease-inherent factors also appear to confer a major risk, indicating that the BMD should be determined in all IBD patients, irrespective of steroid treatment. (Frei,P et al. 2006, `Analysis of risk factors for low bone mineral density in inflammatory bowel disease’, Digestion, vol.73, no.1, pp.40-6)
This study (Sahni,S et al, (2009), Inverse association of carotenoid intakes with 4-y change in bone mineral density in elderly men and women: the Framingham Osteoporosis Study, American Journal of Clinical Nutrition, vol.89, iss.1, pp.416-24) tracked changes in bone mineral density in the hip and lumbar spine in male (213) and female (390) volunteers aged 75 years on average and measured at the beginning of the study and 4 years later. It found that: • There was a link between the intakes of lycopene and the change over 4 years in the BMD of the lumbar spine in women.
Carotenoid intake was linked to changes in the hips of men. BMD in the hips of men were also associated with intakes of total carotenoids, beta-carotene and lutein plus zeaxanthin. • The authors consider that it is possible that the carotenoids can now explain part of the previously observed protective effects of fruit and vegetable intake on BMD.
treatment • Physical activity and body weight: • Physical activity may be the single most important factor supporting bone growth during adolescence. Muscle strength and bone strength go hand in hand. • To maintain healthy bones a person should engage in weight training or weight-bearing endurance activities such as tennis, jogging or vigorous walking regularly.
Regular physical activity combined with an adequate calcium intake helps to maximise bone density in adolescence. • Even past menopause, when most women are losing bone, weight training improves bone density.
Smoking and alcohol: • The bones of smokers are less dense than those of non-smokers – even after controlling for differences in age, body weight and physical activity habits. • Fortunately, these damaging effects can be reversed with smoking cessation. Blood indicators of benefical bone activity are apparent 6 weeks after a person stops smoking. • In time, bone density is similar for former smokers and non-smokers.
Alcohol : • influences fluid excretion leading to excessive calcium losses in the urine; • Upsets the hormonal balance required for healthy bone; • Slows bone formation leading to lower bone density; • Stimulates bone breakdown; • Increases the risk of falling.
Many nutrients are important for building and maintaining healthy bones throughout life calcium, magnesium, phosphorus, protein and vitamins C, D and K. • Calcium, vitamin D and protein are found in milk and dairy products; • Experts recommend that elderly people be exposed to at least 15 minutes of sunlight daily to obtain (make) enough vitamin D; • Magnesium and potassium help to maintain bone mineral density. Magnesium is found in seafood, legumes, nuts and brown rice;
Phosphorus is found in almost all foods, especially good sources of protein; • Broccoli and brussels sprouts are good sources of both vitamins C and K; • Vitamin C is also found in citrus fruits and a variety of other fruit and vegetables, whereas legumes and fish are good sources of vitamin K; • Vitamin D is found in oily fish and, on exposure to sunlight, is made from cholesterol in the skin
Vitamin K deceases bone turnover and protects against hip fractures; • Vitamin a is needed in the bone-remodelling process, but excessive Vitamin A may be associated with osteoporosis; • Omega-3 fatty acids may help preserve bone integrity; • On the other hand, diets containing too much salt are associated with bone losses.
Some substances in foods such as fibre, oxalates and phytates can decrease absorption of calcium. • Phytates are commonly found in whole grains and nuts and oxalates are present in many vegetables, especially green leafy varieties such as spinach and collards. • People with osteoporosis should not consume large amounts of these compounds on a daily basis. • Because these foods are nutrient rich it is advised to continue to eat them but in moderation.
Reference list: Australia’s Health 2010, a publication by the Australian Institute of Health and Welfare, Canberra Jamison,J (2003) Clinical Guide to Nutrition and Dietary Supplements in Disease Management, Churchill Livingstone McGuire,K & Beerman,K, (2007) Nutritional Sciences: From Fundamentals to Food, Thomson Rolfe,S, Pinna,K & Whitney,E (2009) Understanding Normal and Clinical Nutrition 8th Edition, Cengage Whitney,E, Rolfes,S, Crowe,T, Cameron-Smith,D & Walsh,A (2011) Understanding Nutrition, Cengage www.aihw.gov.au