Download
1 / 42
420 likes | 555 Views
Non-Invasive Enteritis and Food Poisoning. FOODBORNE ILLNESS (Bacterial ). Foodborne illness results from eating food contaminated with organisms or toxins Foodborne illness tends to occur at picnics, school cafeterias , and large social functions

E N D
FOODBORNE ILLNESS (Bacterial) • Foodborne illness results from eating food contaminated with organisms or toxins • Foodborne illness tends to occur at picnics, school cafeterias, and large social functions • These are commonly situations in which food may be left unrefrigerated or food preparation techniques are insufficiently safe • Foodborne illness often occurs from undercooked meats or dairy products that have remained at room temperature for extended periods
In patients with foodborne illness, fluid consumption is important to avoid dehydration • Solid foods should not be eaten until the diarrhea has passed, and dairy should be avoided, as it can worsen diarrhea temporarily • Intravenous fluid may be indicated in patients with severe diarrhea who are unable to drink fluids • for example, caused by nausea or vomiting
Most patients spontaneously recover from the most common types of foodborne illness within a couple of days • Antibiotic therapy is usually not indicated, except in cases of severe illness • Infants and elderly people have the greatest risk for foodborne illness • It is estimated that foodborne gastroenteritis causes 48 million illnesses, 127,000 hospitalizations, and 3,000 deaths in the United States annually
VIBRIO • Members of the genus Vibrio are short, curved, rod-shaped organisms • Vibrios are closely related to the family Enterobacteriaceae • They are rapidly motile by means of a single polar flagellum • Vibriosare facultative anaerobes
Pathogenic vibrios include • 1) Vibrio cholerae, serogroup O1 strains that are associated with epidemic cholera • 2) non-O1 V. cholerae and related strains that cause sporadic cases of choleralike and other illnesses • 3) Vibrio parahaemolyticus and other halophilic vibrios, which cause gastroenteritis and extraintestinalinfections
A. Epidemiology • V. cholerae is transmitted to humans by contaminated water and food • Among humans, long-term carriage is considered uncommon • Outbreaks have been associated with raw or undercooked seafood harvested from contaminated waters • Natural (and even man-made) disasters are often followed by cholera outbreaks
B. Pathogenesis • Following ingestion, V. cholerae infects the small intestine • Adhesion factor(s) are important for colonization and virulence • The organism is noninvasive but adheres to the epithelium by expression of pili called Tcp, or toxin-coregulated pili • These pili are coordinately expressed along with cholera toxin, which is an enterotoxin that initiates an outpouring of fluid • This, in turn, causes an outflowing of ions and water to the lumen of the intestine
C. Clinical significance • Full-blown cholera is characterized by massive loss of fluid and electrolytes from the body • After an incubation period ranging from hours to a few days, profuse watery diarrhea (“rice-water” stools) begins • Untreated, death from severe dehydration causing hypovolemic shock may occur in hours to days, and the death rate may exceed 50 percent • Appropriate treatment reduces the death rate to less than 1 percent • Patients with suspected cholera need to be treated prior to laboratory confirmation, because death by dehydration can occur within hours
D. Laboratory identification • V. cholerae grows on standard media such as blood and Mac-Conkey agars • The organism is oxidase positive, but further biochemical testing is necessary for specific identification of V. cholerae
E. Treatment and prevention • Replacement of fluids and electrolytes is crucial in preventing shock and does not require bacteriologic diagnosis • Antibiotics (doxycycline is the drug of choice) can shorten the duration of diarrhea and excretion of the organism • Prevention relies primarily on public health measures that reduce fecal contamination of water supplies and food • Adequate cooking of foods can minimize transmission • Vaccines that are only modestly protective are available in many other countries but not in the United States
ESCHERICHIA COLI • Escherichia coli is part of the normal flora of the colon in humans and other animals but can be pathogenic both within and outside of the GI tract • E. coli has pili that are important for adherence to host mucosal surfaces, and different strains of the organism may be motile or nonmotile • Most strains can ferment lactose in contrast to the major intestinal pathogens • E. coli produces both acid and gas during fermentation of carbohydrates
A. Structure and physiology • E. coli shares many properties with the other Enterobacteriaceae • They are all facultative anaerobes, they all ferment glucose, and they all can generate energy by aerobic or anaerobic respiration
B. Clinical significance: intestinal disease • Transmission of intestinal disease is commonly by the fecal–oral route • contaminated food and water serving as vehicles for transmission • E. coli infection should be suspected in all patients with acute bloody diarrhea • particularly if associated with abdominal tenderness and absence of fever
C. Clinical significance: extraintestinal disease • The source of infection for extraintestinal disease is frequently the patient's own flora, in which the individual’s own E. coli is nonpathogenic in the intestine • However, it causes disease in that individual when the organism is found, for example, in the bladder or bloodstream (normally sterile sites)
D. Laboratory identification • 1. Intestinal disease • Because E. coli is normally part of the intestinal flora, detection in stool cultures of disease-causing strains is generally difficult • Current molecular techniques, such as polymerase chain reaction, may be employed to identify E. coli strains
2. Extraintestinal disease • Isolation of E. coli from normally sterile body sites is diagnostically significant • Specimens may be cultured on MacConkeyagar • Strains of E. coli can be further characterized on the basis of serologic tests
E. Prevention and treatment • Intestinal disease can best be prevented by care in selection, preparation, and consumption of food and water • Maintenance of fluid and electrolyte balance is of primary importance in treatment • Antibiotics may shorten duration of symptoms, but resistance is nevertheless widespread • Extraintestinal diseases require antibiotic treatment • Antibiotic sensitivity testing of isolates is necessary to determine the appropriate choice of drugs
Staphylococcal gastroenteritis • Caused by ingestion of food contaminated with enterotoxin-producing S. aureus • Often contaminated by a food handler • These foods tend to be • protein rich (e.g. egg salad or cream pastry) • salty (S. aureus is salt tolerant) • improperly refrigerated • These heat-resistant toxins are able to withstand subsequent reheating
Symptoms, such as nausea, vomiting, and diarrhea, are acute following • a short incubation period (less than 6 hours) • triggered by the toxin on the GI tract rather than from infection • Staphylococcal food poisoning has short incubation period • the toxin in the food has already been formed before the food is ingested
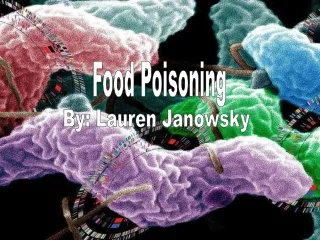
Laboratory Identification • Identification of an isolate as a staphylococcus relies largely on • microscopic and colony morphology • catalase positivity • Bacteria stain • strongly gram-positive • frequently seen in grapelike clusters • S. aureus colonies tend to be yellow • S. aureus is also distinguished from most coagulase-negative staphylococci by being mannitol-positive
Scanning electron micrographof S. aureus; false color added Gram stain of S. aureus cells which typically occur in clusters
Laboratory Identification • Specimens • Stool, vomitus, and food can be tested for toxin and cultured if indicated • Culture • Mannitol salt agar
Immunity • S. aureus infections do not elicit strong or long-lasting immunity • as demonstrated by the continuing susceptibility of individuals to S. aureus infections throughout life
Treatment • Serious S. aureus infections require aggressive treatment including systemic antibiotics • Choice of antibiotics is complicated • by the frequent presence of acquired antibiotic resistance determinants • Virtually all community and hospital-acquired S. aureus infections are now resistant to penicillin G • This has required the replacement of the initial agent of choice, penicillin G, by β-lactamase-resistant penicillins, such as methicillin or oxacillin • However, increased use of methicillin and related antibiotics has resulted in S. aureus that is resistant to a number of β-lactam antibiotics, such as methicillin, oxacillinand amoxicillin • These strains are known as methicillin-resistant S. aureus (MRSA)
Prevention • There is no effective vaccine against S. aureus • Infection control procedures • disinfection of hands and fomites • control of nosocomial S. aureus epidemics
Clostridium perfringens • C. perfringens • large • nonmotile • gram-positive • encapsulated bacillus • It is ubiquitous in nature, with its vegetative form as part of the normal flora of the GI tract • Its spores are found in soil • spores are rarely seen in the body or following in vitro cultivation • Some strains of C. perfringens cause a common form of food poisoning • C. perfringens can cause anaerobic cellulitis and myonecrosis (gas gangrene)
C. perfringens Foodborne Infection • C. perfringens is a common cause of foodborne infection in the United States • Typically, the onset of nausea, abdominal cramps, and diarrhea occurs 8 to 18 hours after eating contaminated food • fever is absent and vomiting rare • attack usually self-limited, with recovery within 1-2 days • occurrence of clinical symptoms requires large inoculum
Typical clostridial enterotoxin food poisoning • cooking that fails to inactivate spores • followed by holding the food for several hours under conditions that allow bacterial germination and several cycles of growth • Vegetative cells are consumed in the contaminated product • C. perfringens then reproduces following ingestion and produces toxin in vivo • Meats, meat products, and gravy are the most commonly implicated foods in C. perfringens foodborne illness
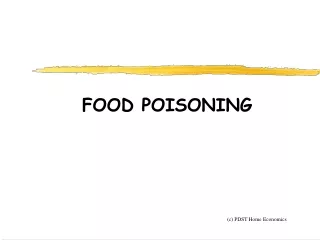
Laboratory identification • In food infection, the organism can be sought in suspected food and the patient's feces • Gram stain and other laboratory findings greatly help planning of antibiotic therapy in patients with clinical manifestations of gas gangrene
Cultures of Clostridium perfringens grown on an egg yolk agar plate Photomicrograph of gram-positive Clostridium perfringens bacilli
Treatment and prevention • C. perfringens is sensitive to penicillin and several common inhibitors of prokaryotic protein synthesis • Because clostridial infections usually involve a mixture of species, the use of broad-spectrum antibiotics is appropriate
Clostridium botulinum • C. botulinum causes botulism, which occurs in several clinical forms • Botulism is caused by the action of a neurotoxin that is one of the most potent poisons known and causes a flaccid paralysis • Contact with the organism itself is not required, and the disease can be solely due to ingestion of toxin-contaminated food
Epidemiology • C. botulinum is found worldwide in soil and aquatic sediments • spores frequently contaminate vegetables and meat or fish • Under appropriate conditions(strictly anaerobic environment, and neutral/alkaline pH) • the organism germinates • toxin is produced during vegetative growth • Because the toxin is often elaborated in food, outbreaks frequently occur in families or other eating groups
Clinical significance:a. Classic botulism (Children and Adults) • Food poisoning in which a patient first begins to experience • difficulties in • focusing vision • swallowing • other cranial nerve functions • 12 to 36 hours after ingesting toxin-containing food • there is no fever or sign of sepsis
A progressive paralysis of striated muscle groups develops • Mortality rate is about 15 percent, with the patient usually succumbing to respiratory paralysis • Recovery, which involves regeneration of the damaged nerves, is protracted, lasting several weeks
b. Infant botulism • The most common form of botulism in the United States today is infant botulism • An infant has yet to develop mature colonic microbial flora • C. botulinum can colonize the large bowel of infants and produce toxin • The botulinum toxin is produced in vivo and slowly absorbed • Constipation, feeding problems, lethargy, and poor muscle tone are common early signs
Supplementation of infant foods with raw honey • which is contaminated with C. botulinum spores, may transmit the organism • The condition is possibly a cause of Sudden Infant Death Syndrome (SIDS) • recovery is the usual outcome • following symptomatic treatment that may be prolonged
Laboratory identification • The organism can be culturedand identified by standardanaerobic methods • Toxin is also identifiablein serum, stool, and food
Treatment and prevention • Antitoxin, which neutralizes unbound botulinum toxin, should be administered as soon as possible in suspected botulinalintoxication • Supportive measures, including mechanical ventilation, may be required • In wound and infant botulism, the infection can be treated with penicillin or other antibiotics to which the organism is sensitive • The toxin is inactivated at boiling temperatures, although killing of botulinal spores requires moist heat under pressure (autoclaving)