Download
1 / 20
220 likes | 1.02k Views
Should we routinely identify the superior laryngeal nerve in thyroid surgery?. Does identification aid in the functional preservation of the nerve?. Overview. Background Anatomy EBSLN Classification System Mechanism of Injury Symptoms of injury Proposed mechanisms of Reducing injury

E N D
Should we routinely identify the superior laryngeal nerve in thyroid surgery? Does identification aid in the functional preservation of the nerve?
Overview • Background Anatomy • EBSLN Classification System • Mechanism of Injury • Symptoms of injury • Proposed mechanisms of Reducing injury • Trial comparing 2 surgical techniques
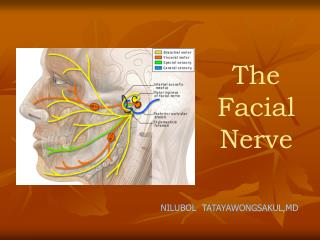
Background • SLN, branch lower end ganglion nodosum of vagus nerve • divides into internal and external branches at ~ level hyoid bone, in close proximity to STA • Internal branch (sensory & autonomic) supplies laryngeal mucosa superior to vocal folds - accompanies SLA to penetrate thyrohyoid membrane • EBSLN (motor) descends behind larynx (superior thyroid vessels) on inferior constrictor before terminating in the cricothyroid muscle
Mechanism of Injury • EBSLN may be stretched by retractor, or transected when these vessels are divided • Incidence of EBSLN unknown • 0-28%
Symptoms of Injury • Hoarseness (slight) • Weakness • Reduced range of pitch volume • Voice Fatigue • singers, professional speakers, lecturers/teachers
Proposed Methods of Reducing Nerve Injury • Skeletization - individual ligation superior thyroid vessels adjacent capsule of gland • Identification of nerve before ligation superior thyroid pole vessels • Use of nerve stimulator or intraoperative nerve monitor
Is the identification of the external branch of the superior laryngeal nerve mandatory in thyroid operation? Results of a propsective randomised studyBellantone et al.SURGERY 2001;12:1055-1059
Identification EBSLN in Thyroid Surgery.Bellantone et al 2001 • 289 consecutive thyroidectomies underwent prospective phoniatric evaluation • random allocation into 2 groups • A=137 (215); STA ligated after identification EBSLN • B=152 (244); STA br’s ligated separately on capsule of gland (NB: no attempt to identify nerve was made)
Exclusion Criteria • Previous neck irradiation • Previous laryngeal/thyroid surgery • Any other anterior cervical operation
Methods • 2 experienced endocrine surgeons • Phoniatric Evaluation of both groups • D -1 • D +2 • 1 month • 6 months • Videostrobolaryngoscopy & spectrographic examination
Surgical technique • Low transverse collar incision • Elevation of platysma flap • Strap m. divided midline and elevated sharply off gland • Early identification of RLN near inferior pole • Visualisation Parathyroid glands
Outcome Assessment • 10 Outcome Measure: • Incidence EBSLN Injury using phoniatric evaluation • 20 Outcome measures: • operative time • duration of hospital stay • incidence of complications; • intraoperative bleeding • postoperative bleeding • wound infection
Results (1) • 7 patients dysphonic postoperatively • 3 in group A, 4 in group B • Phoniatric evaluation revealed unilateral RLN palsy in all cases • VSL and spectrography at 6/12 demonstrated permanent RLN palsy 2 cases (one from each group) • The other 5 cases were normal phoniatrically at 6/12 demonstrating resolution of RLN paresis and thus no evidence of EBSLN injury
Results (2) • 3 patients (1 in group A, 2 in group B) complained of postoperative phonasthenia and decreased range of pitch volume but with normal phoniatric evaluation! • Symptoms resolved spontaneously at 1, 2 and 2.5 months respectively
Results (3) • Asymptomatic patients (both groups) • Spectrography demonstrated absence of voice changes at D2, 1 month and 6 months • Phoniatric assessment showed absence of; • assymetrical mucosal travelling wave • inferior displacement of affected cord • bowing of affected cord • ipsilateral posterior glottic rotation