Download
1 / 1
10 likes | 156 Views
Evaluation of Pain Drugs: Role of Undetected Underlying Sleep Pathologies Barry T. Peterson, PhD*, Jeremiah Trudeau, PhD**, Nathaniel Katz, MD** *Philips Respironics, Bend, OR, **Analgesic Solutions, Natick, MA. Abstract

E N D
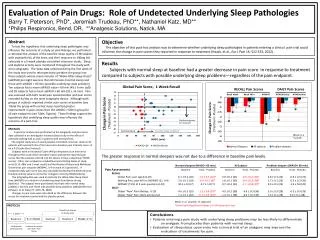
Evaluation of Pain Drugs: Role of Undetected Underlying Sleep Pathologies Barry T. Peterson, PhD*, Jeremiah Trudeau, PhD**, Nathaniel Katz, MD** *Philips Respironics, Bend, OR, **Analgesic Solutions, Natick, MA Abstract To test the hypothesis that underlying sleep pathologies may influence the outcome of a study on pain therapy, we performed a retrospective analysis of the baseline sleep quality of 38 subjects with osteoarthritis of the knee, and their response to 100mg bid celecoxib in a 5-week placebo-controlled crossover study. Sleep and daytime activity were monitored throughout the study with wrist actigraphy. The sleep data collected during the first week of the study was used to retrospectively partition the group into those subjects whose mean minutes of “Wake-After-Sleep-Onset” (aWASO) per night was less than 60 minutes (normal sleep) and those with aWASO > 60 min (possible underlying sleep problem). Ten subjects had a mean aWASO value < 60 min (49 ± 6 min (sd)) and 28 subjects had a mean aWASO > 60 min (92 ± 55 min). Pain was assessed with both recall pain questionnaires and pain scores recorded 4x/day on the wrist actigraphy device. Although both groups of subjects reported similar pain scores at baseline (see Table) the group with normal sleep reported greater improvement in pain scores than the aWASO > 60min group for all pain endpoints (see Table, Figures). These findings support the hypothesis that underlying sleep quality may influence the outcome of a pain trial. Objective The objective of this post-hoc analysis was to determine whether underlying sleep pathologies in patients entering a clinical pain trial could influence the change in pain scores they reported in response to treatment (Haack, et al., Eur J Pain 16: 522-533, 2012). Results Subjects with normal sleep at baseline had a greater decrease in pain score in response to treatment compared to subjects with possible underlying sleep problems—regardless of the pain endpoint. Positive response to treatment Methods A post-hoc analysis was performed on the actigraphy and pain score data collected in an investigator-initiated (Katz) study on the effect of celecoxib (100mg bid) on pain in patients with osteoarthritis. The original study was a 5-week placebo-controlled crossover study on 63 patients with osteoarthritis of the knee and a baseline pain intensity score >4 on a 0-10 scale (See Protocol). Subjects wore an Actiwatch Score (Philips Respironics) on their wrist throughout the study which recorded motion and patient reported pain scores that the subjects entered into the device 4 times a day (Daily “NOW” scores). Other pain endpoints included Numerical Rating Scales at study visits (0-10, 48hr and 1 week recall) and the Western Ontario and McMaster Universities pain subscale (WOMAC, 0-4 on each of 5 questions). A composite daily pain score was also calculated by dividing the NOW value by the daily activity value to correct for changes in activity (NOW/activity). The actigraphy data was used to estimate the Wake-After-Sleep-Onset time (aWASO) as a measure of underlying sleep disturbance during Baseline1. The subjects were partitioned into those with normal sleep (aWASO < 60 min) and those with possible sleep problems (aWASO>60 min) (Ohayon, et al. Sleep 27: 1255-73, 2004). Changes in pain score were calculated as the difference between the scores for treatment period and the placebo period. The greater response in normal sleepers was not due to a difference in baseline pain levels.