Download
1 / 16
160 likes | 184 Views
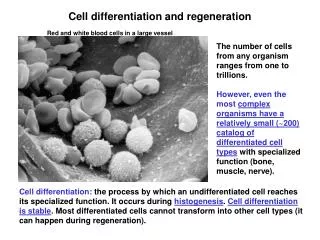
Learn about the dynamics of beta cell mass and regeneration in diabetes, the factors influencing its adequacy, and implications for treatment strategies to maintain glucose homeostasis.

E N D
b cell mass and regeneration Susan Bonner-Weir Translational Working Group on b cell and Islet cell Dysfunction January 10, 2009
Diabetes results if there is an inadequate functional cell mass. This inadequacy can be due to: • destruction (type 1) • functional defect (MODY) • inability to compensate for demand/ insulin resistance (type 2).
In diabetes, b cell mass is reduced to 50% 150 125 6 100 7 75 Cell Mass (% of Lean Control) 4 50 8 25 0 Lean Obese In humans b cell mass increases with obesity Lean Diabetic Obese Diabetic Kloppel G, et al. Surv Synth Pathol Res. 1985;4(2):110-25.
19 16 41 Lean Obese Diabetic Obese IGT Increased b cell volume with obesity in humans In diabetes, b cell mass Is reduced about 50% Mayo series BMI Nondiabetic Lean 22.5±0.5 Obese 36.3±1.3 3 Relative b Cell Volume (%) 2 1 16 30 0 Lean Obese Nondiabetic Butler AE, et al. Diabetes. 2003;52:102-10.
Can a given -cell mass put out much more insulin? Absolutely! With obesity, -cell mass is only 30- 50% increased, but insulin secretory output increased 100%. (24 hr output of insulin: 468 versus 235 nmol) Camastra S, et al. Diabetes 54:2382, 2005 So functional as well as physical increases of cell mass lead to compensation/adaptation.
Non diabetic Insulin requiring diabetic Non-insulin requiring diabetic In vivo measures of b cell function (AIR arginine, AIR glucose and glucose potentiation of AIR arginine) approach 0 when still 40-50% of the b cell mass remains (baboons). McCulloch et al Diabetes 1991
There is a slow continual turnover of b cells with compensation to increased/decreased demand. cell death cell birth Replication (from b cell) • cell mass (Number x volume) Apoptosis Neogenesis (from progenitor or stem cell) b cell volume Hypertrophy vs atrophy
Human islets are 70% b cells and are 1-2% of pancreas 64 yr female, BMI:20.8 Glucagon
Large islets with low % b cells Amyloid deposits with loss of b cells In type 2 diabetes islets have decreasedbcells, due to amyloid formation and loss of cells Glucagon Glucagon insulin Bonner-Weir S & O’Brien T Diabetes 2008 KH Yoon et al, JCEM 2003
b cell mass (total volume) is dynamic cell death cell birth Replication (from b cell) • cell mass (Number x volume) Apoptosis Neogenesis (from progenitor or stem cell) b cell volume Hypertrophy vs atrophy
cell mass is dynamic and is regulated to maintain glucose homeostasis.Marked increases in b cell mass in rodents: • In models of insulin resistance • After glucose infusions • In transplanted islets with induced hyperglycemia • After removal of transplantable insulinoma • After partial pancreatectomy (regeneration) • During pregnancy
Adult human b cells have very low replication rate but can be stimulated to replicate Insulin Ki67 Dapi 45 yr old donor islets transplanted into normoglycemic NODscid mouse
Hormone positive cells budding from ducts = neogenesis Adult human pancreas insulin immunostaining
So, why is the b cell mass in people with type 2 DM only 50% of that of non diabetics with similar BMI?Why is it lower already in IGT? 1. Increased apoptosis 2. Inadequate compensation (replication and/or neogenesis) for increasing insulin resistance 3. Contributions from both 1 and 2 - a minor imbalance will result in a gradual reduction in mass and then loss of function of remaining b cells.
Normal T2DM: Model #2 ?Low birth weight Type 1 DM T2DM: Model #1 Speculation: b Cell Mass During Progression of DM 150 125 100 % 75 50 25 0 30 60 Time (years)
While most of what we know about b cell mass comes from rodents, human b cells have same processes of growth and death. • Actual b cell mass may not be same as functional mass due to effects of hyperglycemia. • Decreased b cell mass already at IFG/IGT suggests that the time for therapies to preserve or replenish is early.