Download
1 / 24
260 likes | 459 Views
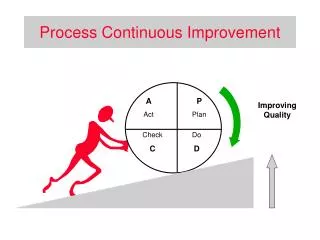
Communicating with oncology patients: a continuous process of adaptation. Esther van Weele Vestalia 14 nov. 2008. Content. Introduction Situations Central issue and central question Model for interaction Advices Conclusion. Esther van Weele .

E N D
Communicating with oncology patients: a continuous process of adaptation Esther van Weele Vestalia 14 nov. 2008
Content • Introduction • Situations • Central issue and central question • Model for interaction • Advices • Conclusion
Esther van Weele • Educational Science (University Twente) + Applied psychology (ITIP) • Self-employed trainer communication and personal effectiveness; Vestalia • Trainer in Oncological Physiotherapy Avans+ • Communicating with oncology-patients (one-day course)
Oncology patients may affect us more than regular patients: • the patient has same age or is younger then yourself • family situation of the patient is similar as yours • the length/intensity of treatment causes more involvement • dealing with intense emotions • dealing with decline and/or death • the complexity of cancer, process • unfamiliarity with (side)effects of cancer treatment • you’re prejudiced regarding a coping style, you have irrational thoughts of coping styles
What if? • Your patient constantly talks about the journey to the far East he wants to make, while you’re certain it will be impossible for him given his condition How would you feel? What would you say? What would you do?
What if? • Your patient in palliative phase doesn’t want to exercise anymore, while you think it is very helpful for him How would you feel? What would you say? What would you do?
What if? • Your patient is very emotional these last weeks, you’re almost not able to continue the treatment How would you feel? What would you say? What would you do?
What if? • Your patient doesn’t want to talk about his nearby death at all, your conviction is that is very helpful to do so How would you feel? What would you say? What would you do?
What if? • Your patient mentioned between nose and lips that she has sexual problems. How would you feel? What would you say? What would you do?
What if? • Your patient, the same age as you have, suffers from major setbacks in her disease process and she finds it very difficult to accept. How would you feel? What would you say? What would you do?
How would you (possibly) feel? • frustrated, irritated, angry • desperate, helpless, unable to do the right things • sad, emotional, compassion • worried, doubting, confused, ashamed • very much involved (thinking about the patient at night), not letting go of a patient • insecure
What would you probably say/do? • How more intense your feelings, how more you get in the grip of the situation. • When you’re in the grip you’ll only use the skills you know best (instead of your whole potential), that feels safe. • And you will use these skills more to influence the situation
Central Issue • Your professional paradigm is about: helping people, treating and activating them, promoting health and movement, helping with their participation and quality of life, giving them attention • If you’re affected by the situation you probably will help/give more and try to influence the situation that way (excercises, suggestions, advices, attention) • But it doesn’t have as much effect as possible (your patient may not react on your effort, your feelings will not go away, your interactionis not effective.)
Central Question • How can you adapt more to situations that affect you so that you can keep control over your own emotions, use your whole capacity of skills and most of all help your oncologypatienteffectivly?
Model Interaction Styles • Model designed by Ferdinand Cuvelier (Belgian psychologist and philosopher). • 6 Styles of Interaction • 80% of the interaction is performed in 2 Styles: Giving and Taking
Giving and Taking Giving offering presenting approaching Information Guidlines Service Goods Precense Person Precense Person Taking/Asking accepting receiving acknowledging Service Goods Information Guidlines
Advice 1: switch to precense • Giving treatment (service, excercises, goods) is equal as good as ‘giving’ and ‘taking’ precense (respectful approach, true personal contact, pick up signals, (emotional) support). • Precense is not about solving problems • Oncology patients expect emotional support • Naming emotions, inviting to talk about what bothers is brave but it is very effective on processing the cancer process! • Sharing your own feelings might be effective as well (‘giving person’) • Switching between the aspects of giving is psychosocial caring!
Situations: • Your patient is very emotional these last weeks, you’re almost not able to continue the treatment(emotions are necessary in processing) • Your patient mentioned between nose and lips that she has sexual problems (picking up a signal, speak shortly about it, refer to sexologist).
Advice 2: adapt more often • Switch more often to Taking (accepting, acknowledging) or Asking (what is most important for you at this moment? what is your goal today?) • Adapt to your patients needs, wishes, moods, copingsstyles (let go of your ‘negative’ convictions) • By taking/asking you give your patient space which helps him processing and it has a positive effect on your trustfullness and interactions • Switching to taking/asking will create more distance of your own emotions/involvement/thoughts
Situations: • Your patient constantly talks about the journey to the far East he wants to make, while you’re certain it will be impossible for him given his condition (acknowledge CS) • Your patient don’t want to talk about his nearby death at all, your conviction is that is very helpful to do so(acknowledge Coping Style) • Your patient in palliative phase doesn’t want to exercise anymore, while you think it’s very helpful for him(accept) • Your patient, the same age as you have, suffers from major setbacks in her disease process and she finds it very difficult to accept (ask her what she expects from you)
Advice 3: you make the change • Do not try to ‘change’ your patient/the situation but try to make a change/ movement yourself • In taking care of yourself and taking responsibility for your own feelings and actions, you will be a physiotherapist that can give your oncology patient the best support and service.
Conclusion In being a professional working with oncology patients your value is added if you’re able to: • Acknowledge/accept the patients’ mood, copingstyle, needs in spite of your own emotions and convictions • Switch between treating, giving information and presence (and value these aspects) • Take responsibility for your own feelings and influence.
Distance Keeping Keeping for himself restraining not giving Giving offering presenting approaching Attacking Confrontating stating critisizing Against Together Keeping off Stopping refusing defending saying “no” Taking/Asking accepting receiving acknowledging Discharging Undergoing Coming over you doubting Distance Model Interaction Styles