Nutrition
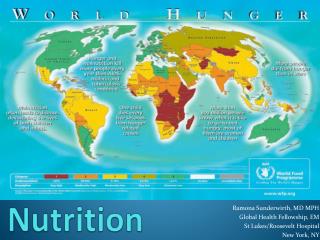
Nutrition. Ramona Sunderwirth, MD MPH Global Health Fellowship, EM St Lukes/Roosevelt Hospital New York, NY. objectives. General principles Specific nutrients Life cycle approach to nutrition Measures of malnutrition Severe malnutrition. Hunger is a term which has three meanings.

Nutrition
E N D
Presentation Transcript
Nutrition Ramona Sunderwirth, MD MPH Global Health Fellowship, EM St Lukes/Roosevelt Hospital New York, NY
objectives • General principles • Specific nutrients • Life cycle approach to nutrition • Measures of malnutrition • Severe malnutrition
Hunger is a term which has three meanings • Uneasy or painful sensation caused by want of food; craving appetite, the exhausted condition caused by want of food • Want or scarcity of food in a country • A strong desire or craving • World hunger refers to the second definition • The related technical term is malnutrition.1 • Malnutrition is a general term that indicates a lack of some or all nutritional elements necessary for human health • Underweight, Stunting, Wasting • Obesity
Major Causes of Death in Children Under Five in Developing Countries and the Contribution of Malnutrition
Causes of Hunger • Poverty – principle cause • Lack of resources, unequal distribution resources (Amartya Sen) • Harmful economic systems → poverty & hunger • control over resources & income based on military, political & economic power that typically ends up in the hands of a minority, who live well, while those at the bottom barely survive, or don’t • Conflict → poverty & hunger • Displaced: refugees & IDP • Hunger → poverty → hunger • poor health, ↓ levels of energy, mental impairment, ↓ ability to work & learn → greater hunger
Causes of Hunger, cont. • Dietary practices • Breastfeeding • Single source diets (corn, rice, cassava) • Lack of education/knowledge or access • Agricultural productivity • lack of farming skills , technology or resources (nitrogen, fertilizers, pesticides , irrigation) • Climate change • current & future cause of hunger & poverty • ↑drought, flooding, changing climatic patterns requiring a shift in crops / farming practices not easily accomplished
Nutritional determinants of healthamong the most powerful environmental factors influencing health & disease • Recommended nutrient intakes • RDA now DRV (dietary reference values) • Food based dietary guidelines • Food pyramid • Malnutrition modulates other diseases • Infection • Major contributor to death • Immunity and malnutrition • Immunity greatly compromised • Barrier defenses breached, cell-mediated immunity depressed • Lymph glands/thymus atrophic • IgA, complement components , phagoycytic activity depressed • Effects of less extreme malnutrition/nutrient deficiencies
Essential Nutrients Energy • Drives consumption of all other nutrients • Intake balanced w/ expenditures • Deficit must be met by body stores • Short term: muscles/liver glycogen/ short term fat stores • Medium term: adipose tissue • Long term: protein • Wasting: sustained energy deficits • Adults: Chronic Energy Deficiency CED (BMI < 18.5) • Famines/poverty • Incorrect child feeding practices • Anorexia of infection & illness
Essential nutrientsCarbohydrates Most energy in most diets (17.6kJ/g) • Amylase, sucrase, maltase, lactase → glucose • Glucose: used by tissues, stored in liver/muscle (glycogen) • Insulin vs Cortisol/GH • Brain consumes 60% of total circulating glucose • Ketones used during starvation (B-hydroxybutyric acid from fats)
Clinically significant disturbances in carbohydrate metabolism • Malabsorption • Lactase deficiency, gut infections, Kwashiorkor, persistent gastroenteropathy • Disturbed Metabolism: hypoGlycemia • Inadequate stores • Marasmus, Kwashiorkor • Liver damage, hepatitis • Sepsis • Toxins/drugs • Alcohol, insulin • Cerebral malaria • Disturbed Metabolism: hyperGlycemia • Hormonal • DM (insulin resistance) • Excess corticosteroids
Essential nutrientsFats (TG) (39 kJ/g) • Saturated (animal) vs Unsaturated (plants) • Long chain PUFAs (breast milk) & EFAs (found only in food) • In Times of Plenty: TG stored in adipose tissue (insulin) • In Times of Negative Energy Balance: • Noradrenaline & GH stimulate Lipase in adipocytes • Fat deposits depleted • EFA & TG oxidized in liver to acetoacetic acid (used for energy) • EFA used directly by skeletal & heart muscle
Disturbances in Fat metabolism • Inadequate stores • Dietary • Starvation, Marasmus • Malabsorption • Infections in Gut (giardia, strongyloides) • Bile salt deficiency • Obstructive Jaundice, Gall bladder disease, • Bacterial overgrowth • Pancreatic damage • Kwashiorkor • Pancreatitis • Disturbed metabolism • Fatty Liver • Kwashiorkor • Alcoholism
Essential nutrientsProteins (17kJ/g) • Provides AA for synthesis: enzymes, plasma proteins, milk, tissue cells • Starvation: AA → glucose (gluconeogenesis)>→decrease muscle mass/ damage to vital organs (Marasmus) • Essential AA found in diet only • Quality of dietary protein measured by animal growth • Animal protein: first class protein, similar AA composition to humans • Milk: high net protein utilization index (NPU=biological value (quality + digestibility) • Plant protein: variable digestibility + quality • plant mixtures can supplement each other (high quality proteins) • Protein concentration in diets • 5-6% energy • 6-8%: infants, malnourished children, lactating women
Clinically important disturbances in protein metabolism • Inadequate stores • Starvation • Marasmus, Kwashiorkor • Malabsorption • Pancreatic disease • Kwashiorkor • Increased catabolism • Infections • Tumours • Inadequate synthesis • Cirrhosis of liver • Diabetes • Increased loss • Nephrotic syndrome • Severe gut infections • Measles, amoebiasis • Bacillary dysentery • Burns & exudates
Essential Nutrients • Minerals • Contained in all tissues/fluids, mainly in bone • Functions in co enzymes, hormones, vitamins • Balanced diet provides adequate amounts • Calcium/Iron: meat/fish/eggs/diary products • Iodide, fluoride, selenium: uptake by plants from soil/rocks • Potassium/magnesium: cardiac/renal diseases & Kwashiorkor/ chronic diarrhea • Micronutrient Initiative (2002): eliminate “hidden hunger” – most damaging worldwide • Iron, iodine deficiency , Vit A
Essential Nutrients • Vitamins • Minute amounts vital for life • Not synthesized in body (except Vit D): obtained in diet • Regulators of metabolic reactions • Fat soluble: Vit A,D,E, K • Water soluble: Vit C, B complex • Deficiencies : • Together in people on poor, monotonous diets • Lack of dairy products (riboflavin); Vit A, Vit C (seasonal) • Emergencies (famines), prisons • Illness w/ suppressed food intake • Cultural: women/infants kept indoors
Life cycle approach to nutrition • Special needs at special times • Phases are linked, and each affect next stage of development: continuous loop Cause & Effect • “Fetal & infant origins of diseases” & “Thrifty phenotype” • Inter generational cycle of malnutrition
Fetal Growth & nutritional needs of pregnant women • Low birth weight • Nutritional effects on fetal growth • Nutritional needs of pregnancy • Dietary supplements in pregnancy • Lactation
Fetal growth & nutritional needs of pregnant women • Low birth weight predictor of NN & post NN mortality • Interventions that raise BW by 100 g have major impact on mortality • Fetal growth influenced by many factors • Woman’s size predictor of BW (S. Asia vs African SGA rates) • Maternal wt gain in pregnancy : 1.5 kg/mo • ↑normal energy intake by 10% (remarkable maternal energy sparing mechanisms) • Nutritional needs of pregnancy & dietary supplements • Community-wide dietary supplementation of poor rural women can enhance BW (Gambia) • HIV + women given micronutrient supplementation : ↓ SGA • Interventions to prevent fetal growth retardation targeted at specific pop.
Lactation • Nutritional requirements of infant > fetus • Energy requirements lactation > pregnancy • Highly “robust” process • Needs to increase energy intake by 20-25% • If balanced diet, other nutrient needs met • Water soluble vitamins, minerals (calcium) • Maternal deficiencies reflected as low concentrations in milk • Fat soluble vitamins • Better buffered • Protein, fat, carbohydrate composition very constant • Supplementation: in extreme situations
Infant Nutrition • Growth • Causes of growth failure • Severe forms of PEM • Classifications: Gomez vs Wellcome • Marasmus • Kwashiorkor • Breast-feeding • Optimal duration of exclusive breast feeding • Weaning foods
Infant Growthwhere food supplies insecure, diet low quality, infections frequent • Breast-fed infants (3-4 mos) • Ideal food, adequate amount, protection from infection • WHO recommends exclusive BF till 6 mos age • Growth faltering • Begins w/ weaning: low nutrient density, contaminated • By 1yr average WFA -2Z score in many areas Africa • If stunted as well as wasted, look better nourished • Strongly associated w/ developmental deficits • “Road to Health” charts • Wasting: acute malnutrition • Stunting: longer term deficit
Malnutrition • WHO defines malnutrition as the cellular imbalance between the supply of nutrients & energy & the body’s demand for them to ensure growth, maintenance, & specific functions.
Protein energy malnutritionPediatrics • Wasting : acute malnutrition • Rapid weight loss or failure to gain weight normally • Stunting: chronic malnutrition • Failure of linear growth • Underweight: acute & chronic malnutrition • occurs as a result of wasting, stunting, or both
Nutrition & Malnutrition • Child
Malnutrition ClassificationsChronic Malnutrition → StuntingEventually affects child’s body proportions → Wasting • Gomez Classification: • The child's wt compared to that of a nl child of the same age • Useful for population screening & public health evaluations • % of reference wt for age = [(patient wt) / (wt of nl child of same age)] • Waterlow Classification: • % wt for ht = [(wt of patient) / (wt of a nl child of the same ht)] • % ht for age = [(ht of patient) / (ht of a nl child of the same age)]
Wellcome Classificationevaluates the child for edema & with the Gomez Classification system Wt for Age (Gomez) w/ Edema w/ out Edema • 60-80% Kwashiorkor Under nutrition • <60% Marasmic- Marasmus Kwashiorkor
Malnutrition Classifications • Gomez- Public Health screenings & Emergencies • WFA% (reference) Classification • 90-110 Normal • 75-89 Grade I – Mild • 60-74 Grade II – Moderate • <60 Grade III - Severe • Wellcome – Clinical Settings • WFA% (NCHS median) No edema With edema • 60-80 Undernutrition Kwashiorkor • < 60 Marasmus Marasmic/ Kwashiorkor
Methods of assessing growth failure & pediatric malnutrition • Reference growth curves for Wt & Ht • Road to Health: %WFA %HFA %WFH ( if age unknown) • Expected wt/ht for age WHO curves in Africa • Centile curves • Same reference curves, 50% is line up center distribution Nl population • Z-scores • 1 SD from mean of Nl population (average WFH O Z-score) • Applied to WFH, HFA, WFA • MUAC: constant from 1-5 yrs ag • >140: Normal , 115-140 mild/moderate, <115 severe • Red-severe acute Orange-moderate acute Yellow refer Green- Nl • HC, Skinfold thickness (triceps & supra-scapular)
Causes of growth failure • Infections • Primary nutrient shortages-seasonal, famine, cultural, conflict • Tropical gastroenteropathy • Villous atrophy: degree predicts growth • Affects nutrient absorption (lactose) • Loss of plasma proteins: protein enteropathy (measles) • Increased permeability • Over active inflammatory response
Malnutrition in Children • 25% world’s pediatric pop undernourished • Contributes to > 50% U5 Mortality in RPC • Children very vulnerable to malnutrition • High nutritional requirements for growth • Reliance on others for food access • Two classic phenotypic presentations • PEM + micronutrient deficiencies • Marasmus: decreased WFH + severe wasting • Kwashiorkor: distinguished by edema • Marasmic/Kwashiorkor : elements of both
Pathophysiology • Tissue starvation influences physiology at every level • Native & acquired immunity weakened • Antioxidant deficiencies → unchecked free radicals to inflict direct cellular damage • Injury to cell wall Na-K pumps → Na retention & K wasting • HypoGlu: exhaustion of muscle glycogen stores & impaired gluconeogenesis • Atrophy & oxidant induced damage of myocardial tissues → cardiac dysfunction + • Fluid shifts from leaky membranes + large Na loads during recovery → CHF
Severe forms of Malnutrition • Marasmus • “adapted state”: prolonged underfeeding forces child to consume own fat/protein stores to maintain function vital organs • 1st yr of life, WFA & HFA diminished • Thin, severe muscle wasting, weak • Sunken eyes, dry mucous membranes, skin tenting, decreased tears : not to be confused w/ dehydration • Bradycardia, hypo TA & hypothermia • Thin, dry skin, redundant skin fold. Thin, sparse hair, easily plucked
Severe Forms of Malnutrition • Kwashiorkor • “Disadapted state”, imbalance in protein supply limits hepatic production albumin & plasma proteins → edema • 2nd year of life. Acute illness • Marked muscle atrophy, w/ nl body fat. Anorexia. Apathetic, irritable • Pitting edema, anasarca, “Moon Face” • Dry, atrophic, peeling skin, confluent areas of hyperkeratosis & hyper pigmentation: Flaky paint dermatosis • Dry, dull, hypopigmented hair, orange, falls out/easily plucked • Hepatomegaly (fatty liver infiltrates)+ dilated/hypomotile intestinal loops + bacterial overgrowth/gas production, weak abd muscles → distended abdomen
Childhood & adolescence • Higher metabolism rate /energy/nutrient requirements than adults • Adolescent growth spurt energy, protein, Ca & Iron requirements raise • Same diet as Adults • Often fed last, after Men, Women & younger children
Treatment of Malnutrition • For another Thursday