Download

1 / 14
140 likes | 153 Views
Explore the latest data on robotic procedures, surgeon skills impact, and future technologies. Uncover results of comparative studies and surgical skill influence on patient outcomes for various surgeries. Assessment of surgeon and hospital experience on robotic partial nephrectomy. Discover the impact of techniques on outcomes in robotic radical nephrectomy with inferior vena cava thrombectomy.

E N D
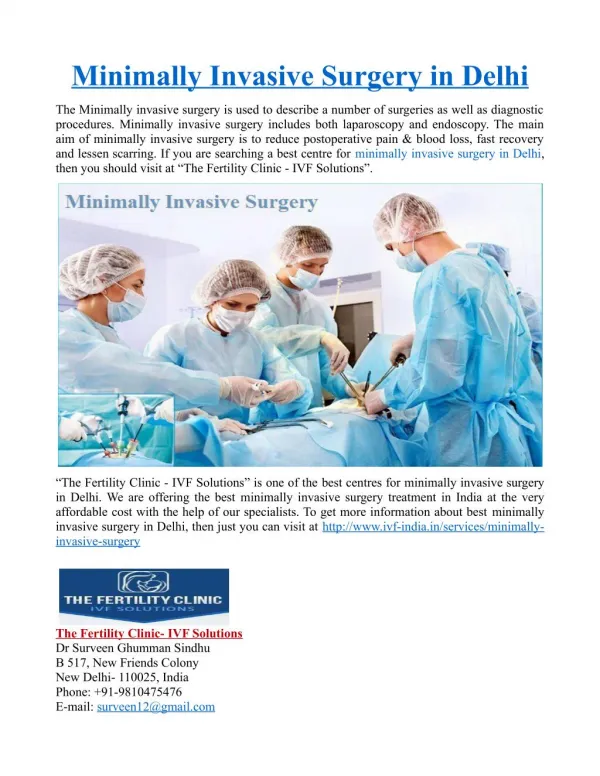
Take Home Messages Minimally Invasive Surgery Robotics and Laparoscopy Fernando J. Kim, MD, MBA, FACS Chiefof Urology, DHMC Professor of Surgery/Urology, UCDenver
RosaliaViterbo MD, Facs Fox Chase Cancer Center Philadelphia, Pa Monish Aron, MD Professor Of Urology & Vice-chair, Clinical Operations University Of Southern California, Los Angeles Li-ming Su, M.D. Chairman, Department Of Urology David A. Cofrin Professor Of Urologic Oncology University Of Florida College Of Medicine Stephen A. Boorjian, MD Carl Rosen Professor Of Urology Vice Chair Of Research Director, Urologic Oncology Fellowship Department Of Urology Mayo Clinic, Rochester, MN Erik P. Castle, M.D., F.A.C.S. Professor Of Urology Urologic Oncology Mayo Clinic Phoenix, AZ
Highlight podium/poster/video/plenary sessions • Maturing and emerging data on robotic procedures • Continued emergence of new applications using the minimally invasive platform • Association of surgeon skills and patient outcomes • Interest in novel training concepts and education • Future technologies to help aid in the Minimal Invasive approach
RARP: COMPARATIVE EFFECTIVENESS • PD15-07 ERECTILE-FUNCTION AND ONCOLOGIC OUTCOMES AFTER OPEN RETROPUBIC AND ROBOT-ASSISTED RADICAL PROSTATECTOMY: RESULTS FROM A LARGE, PROSPECTIVE SWEDISH TRIAL Sooriakumaran et al, Stockholm, Sweden • Prospective trial looking at open vs. robotic prostatectomy across Sweden • 14 centers, surgeons having done >100 cases • Multiple data points, patient reported EF, surgeon reported extent of NS, potency rates and biochemical recurrence at 2 yrs • pT2 margin rates better for open than robot: No difference in BCR for pT2 disease • pT3-4 margin rates worse for open than robot: Worse BCR for pT3-4 disease with open • No difference for D’Amico high risk patients, low and intermediate risk men had improved potency recovery at all time points with robotic vs open surgery Take Home: Quasi-randomized trial: outcomes favor robotic approach. Caution: limited short term follow up of 2 years.
RARP: SUGICAL SKILL • PD58-06 SURGICAL SKILL AND PATIENT OUTCOMES AFTER ROBOT-ASSISTED RADICAL • PROSTATECTOMY Peabody et al, Ann Arbor, MI • MUSIC (Michigan Urological Surgery Improvement Collaborative) • Assess association between peer review of technical skill and short term operative outcomes in RARP • Surgeons performing RARP in MUSIC submitted video clips of NS RARP • Edited clips of the vesico-urethral anastomosis from 29 surgeons underwent blinded review • Each surgeon underwent video review by at least 9 peer surgeon reviewers • Surgeons were ranked on global robotic skills using GEARS scores (Global Evaluative Assessment • of Robotic Skills (GEARS) tool using a custom designed web-based secure registry • Surgeon in the lowest 25% quartile of skill ratings were compared to surgeons in the top 25% quartile and higher quartile surgeons had lower rates of estimated blood loss and less events of catheter replacement • No differences in readmission rates or prolonged catheter duration outcomes. • Technical skill of surgeons performing anastomosis during RARP varied widely Take Home: Better skills associated with better results.
RAPN: SURGEON /HOSPITAL VOLUME AND PATIENT OUTCOME • PD09-12 THE IMPACT OF SURGEON AND HOSPITAL EXPERIENCE ON THE PERIOPERATIVE • OUTCOMES OF PATIENTS RECEIVING ROBOTIC PARTIAL NEPHRECTOMY Khandwala, San Diego, CA • All-payer hospital clinical and economic database queried • 50,282 patients who underwent RAPN were identified from 2003-2015 • Surgeon and hospital RAPN volumes were calculated & divided into low/medium/high volume quartiles • Results: • Higher volume surgeons and hospital had increased rate of older pts., academic, >500 beds, urban settings • Higher volume surgeons had fewer overall complications, and major compared to Lower volume surgeons • Total cost of stay was not significantly different regardless of surgeon or hospital experience Take Home: Increased experience in RAPN by both surgeon and hospital associated with lower complication rates and shorter LOS, but in hospital cost not significantly affected by provider experience.
RAPN: TECHNIQUE AND OUTCOME • PD04-06 ROBOT ASSISTED RADICAL NEPHRECTOMY AND INFERIOR VENA CAVA • THROMBECTOMY: SURGICAL TECHNIQUE, PERIOPERATIVE AND ONCOLOGIC OUTCOME. • Simone, Rome, Italy • 35 consecutive patients with renal tumor and IVC thrombus were treated between • July 2011 and September 2016. • 2 tertiary hospitals • Technique highlighted perioperative and oncologic outcomes • intracorporeal robot-assisted radical nephrectomy with • IVC level I (5.7%) II (65.7%) and III (28.6%) tumor thrombus Take Home: Robotic IVC thrombectomy is challenging, in tertiary referral centers this procedure is feasible, safe and associated with favorable perioperative outcomes and encouraging short term oncologic outcomes.
Minimally Invasive Adrenalectomy: OUTCOMES • MP37-11 LAPAROSCOPIC VS. OPEN ADRENALECTOMY: UROLOGIC OUTCOMES FROM A • NATIONAL PROSPECTIVE DATABASE Lu et al, Boston MA • ACS-NSQIP Participant (2007-2012) were queried • Prolonged length of stay (pLOS), prolonged operative time (pOT), 30-day complications • (including infectious, thromboembolic, renal, cardiac, pulmonary, and neurologic events), and need for • blood transfusion, re-intubation, or reoperation • 291 patients who underwent adrenalectomy were identified (urologist only) • 73 underwent open and 218 underwent laparoscopic elective adrenalectomy • Results: Laparoscopic approach was utilized more for pts. with BMI of >25, and was not associated with ASA score • overall complication rate was 6.2%: 9.6% for open and 4.6% for laparoscopic • laparoscopic adrenalectomies were associated with shorter operative time, and LOS, postoperative dvt and decreased need for blood transfusions. Take Home: Lap adrenalectomy is faster, results in shorter LOS, & complication rate. Comparable 30-day post-operative outcomes. Lap Ax should be attempted when possible.
RPLND: SURGICAL TECHNIQUES • V6-02 POST CHEMOTHERAPY ROBOTIC RETROPERITONEAL LYMPH NODE DISSECTION FOR NON-SEMINOMATOUS GERM CELL TUMOR. /PENARY SESSION Porter et al. Seattle, WA • Present their technique of R-RPLND using both the daVinci Si and Xi robot. • full bilateral dissection with Nerve sparing were performed • 4 patients diagnosed with NSGCT that had completed 3-4 cycles of BEP, and noted to have retroperitoneal masses with normal tumor markers. • Mean operative time was 339. Mean estimated blood loss was 125cc. Mean number of lymph nodes excised was 28. There were no transfusions and no open conversions. • R-RPLND in the PC setting is feasible and offers patients the benefits of a minimally invasive approach, but is technically challenging. Take Home: NEED FOR MORE RCT, less regionalization and more cooperation, and to be PRO-Responsible when doing these technically challenging procedures.
TRAINING AND EDUCATION: IMPROVING PATIENT OUTCOMES • PNFBA-02 TECHNICAL SKILL ASSESSMENT OF SURGEONS PERFORMING ROBOT-ASSISTED RADICAL PROSTATECTOMY: RELATIONSHIP BETWEEN CROWDSOURCED REVIEW AND PATIENT OUTCOMES Ghani et al, Ann Arbor Michigan • Pilot study from the Michigan Urological Surgery Improvement Collaborative (MUSIC) • To assess the association between crowd sourced (lay person) video rating review of surgeon • skill with short term outcomes following RARP • Crowdsourcing: a process of obtaining input into a task by using large groups of decentralized, independent people providing aggregated feedback, often online • MUSIC Participants: 43 practices, 260 urologists, registry of 34,000 patients, and >8,000 RARP • Online crowdsourced reviewers agreed with experts on the rank order of sugeons with the lowest skill scores • Higher skilled surgeons had significantly lower complication rates Take Home: Crowdsourcing could serve as a filter through which lower performing surgeons are identified for peer review and coaching/teaching inititatives. Better skills may lead to improved patient care.
RARC: COMPARATIVE EFFECTIVENESS • PNFLBA-18 A PROSPECTIVE, MULTICENTER, RANDOMIZED TRIAL OF OPEN VERSUS • ROBOTIC RADICAL CYSTECTOMY (RAZOR) Parekh, et al Coral Gables, FL • 1st Phase 3 Multicenter prospective randomized trial comparing open to robotic approach for organ site • 350 patients with clinical stage T1-T4, N0-N1, M0 or CIS refractory bladder cancer were randomized • 1:1 to ORC or RAsRC across 15 US institutions, 2011-2017 • The RAZOR trial compares open versus robotic cystectomy using • oncologic, perioperative, functional and QOL endpoints. • Trial designed as a non inferiority comparison, with RARC • being considered inferior if 2yr PFS was >15% lower than ORC • Other endpoints • complications (using Clavien-Dindo system), LN yield, and margin status Take Home: Robotic approach associated with shorter LOS, lower EBL, and transfusion rates, than ORC. Overall surgical margins and LN yield similar in both groups. However, increased bladder soft tissue margin and increase operative times for robotic group. “RCT in minimally invasive arena “CAN BE DONE!”
FUTURE TECHNOLOGIES • PD10-06 INTRA-OPERATIVE OPTICAL IMAGING UTILIZING ANTI-PSMA (PROSTATE SPECIFIC MEMBRANE ANTIGEN) FLUORESCENT ANTIBODY DURING ROBOT ASSISTED RADICAL PROSTATECTOMY (RARP) Chennamsetty, et al Duarte, CA • First In-vivo study using anti PSMA antibody with a conjugated fluorescent marker (to help identify prostatic tissue) • Specificity against PSMA may help guide preservation of critical structures: • NS and to help avoid positive margins or identify potential metastatic sites • Objective: To investigate dosing/timing and Correlate intraoperative findings • 5 Patients received IV MDX-1201 four days prior to RARP • A 488 nm laser was attached to da Vinci Si surgical robot camera • 5 mg dose for first three patients-failed to show fluorescence • Escalated 15mg dose in 4th patients: ex vivo fluorescence in prostate tissue • 5th patient: showed in vivo fluorescence of prostate tissue, although a false positive LN was seen that was pathologically negative Take Home: 1st in human study using anti PSMA Ab demonstrating real time fluorescence to help guide preservation of critical structures.
HOW TO PREVENT? Sotelo RJ et al, EurUrol 2016