Download
1 / 13
140 likes | 367 Views
Applying a Health Equity Lens Presentation at Gender, Diversity & Women’s Health & Well-being ~ A Manitoba Research Day February 11, 2013. Marcia Anderson DeCoteau, MD MPH FRCPC Medical Officer of Health Karen Serwonka , BA MHSc Cert HIA Senior Policy Advisor Health Equity Unit

E N D
Applying a Health Equity LensPresentation at Gender, Diversity & Women’s Health& Well-being ~ A Manitoba Research DayFebruary 11, 2013 Marcia Anderson DeCoteau, MD MPH FRCPC Medical Officer of Health Karen Serwonka, BA MHSc Cert HIA Senior Policy Advisor Health Equity Unit Office of the Chief Provincial Public Health Officer Manitoba Health
What do we mean by Health ? “Health is: living in a community where basic necessities are affordable and the community is set up and safe so that people can be active, eat healthy and keep themselves and their community clean. Traditional ways are respected and supported and the role of parents and families is strengthened. The community is independent and has strong leadership that engages community members and advocates for better social and environmental conditions and safe and accessible health care” Garden Hill First Nation 2
What do we mean by Health Equity ? Health equity is an aspirational goal where all people, regardless of gender, race, income, class, or sexuality have an equal opportunity to be healthy. (Anderson DeCoteau, 2012) Achieving health equity requires challenging and changing the unfair and steeply graded distribution of social resources to which everyone has equal claims and rights. (World Health Organization, Commission on the Social Determinants of Health, 2008) 3
What do we mean by Health Inequities ? “Health inequities refer to a subset of health disparities or inequalities that are systematically associated with underlying social disadvantage (e.g., by virtue of being poor and/or a member of a disenfranchised or marginalized group). They reflect unequal opportunities to be healthy, and thus, are considered avoidable and unfair.” (Braveman & Gruskin, 2003) • while all health inequities can be considered to be health inequalities / /disparities, • not all health inequalities/disparities are considered to be health inequities.
Health Inequity: International Context World Health Organization Commission on the Social Determinants of Health. (2008). http://www.who.int/social_determinants/thecommission/finalreport/en/index.html WHO Commission on the Social Determinants of Health (CSDH) • released final report in 2008 • implores us to address health inequities by tackling the inequitable distribution of power, money and resources World Conference on SDoH • 2010 in Brazil • adopted the Rio Political Declaration • identifies shared responsibility for health equity be acted upon through “all for equity” and “health for all” global action • across sectors and government departments • all levels of government • in collaboration with and supporting civil society involvement • ensuring corporate social responsibility
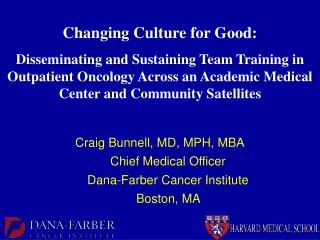
Diverse population groups … diverse determinants Another Important Indigenous Conceptual Framework Source: www.healthnexus.ca/projects/primer.pdf as noted in UNICEEF. 2007. Canadian Supplement to the State of the World’s Children 2009. Aboriginal children’s health: Leaving no child behind. http://www.who.int/social_determinants/knowledge_networks/add_documents/mekn_final_guide_112007.pdf 6
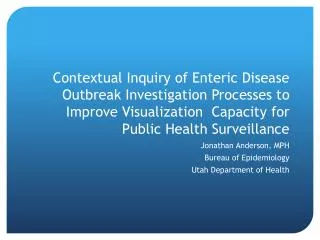
Intervening downstream , midstream or upstream ... how much of an impact will we have? Midstream interventions “ seek to reduce risky behaviours or exposures to hazards by influencing health behaviours or psychosocial factors and/or by improving material working and living conditions … (They) generally occur at the community or organizational level.” Upstream interventions “include reform of fundamental social and economic structures and involve mechanisms for the redistribution of wealth, power, opportunities, and decision-making capacities … (They) typically involve structural and system-level changes.” r Downstream interventions “ occur at the micro and/or individual level and mitigate the inequitable impacts of upstream and midstream determinants through efforts to increase equitable access to health care services.” What is the appropriate balance to fulfill Manitoba Health’s Vision ? : Healthy Manitobans through an appropriate balance of prevention and care. Source for visual: PP Presentation: Transforming Services: An Assets Based Approach. Karen Grieve, Scottish Government, Health Inequalities Branch. Source for definitions: National Collaborating Centre for the Determinants of Health. 2012. Assessing the Impacts and Effectiveness of Intersectoral Action on the SDoH and Health Equity: An Expedited Systemic Review. 7
Health Equity: Provincial Context Chief Provincial Public Health Officer’s Report on the Health Status of Manitobans 2010 Goals: • Improved health of Manitobans • Reduced inequalities of health among Manitobans Recommendation 3.1: “It is recommended that the Manitoba government, including all departments, relevant crown corporations and funded agencies ... adopt methods to assess the impact of major decisions, policies, legislation and other actions on the health of Manitobans and the inequalities of health of Manitobans.” 8
A commitment to change • Health is influenced by the type of society we choose • No one is immune to health problems and health inequalities – everyone is affected • Many policies and programs are making a difference in the lives of Canadians and are contributing to a reduction in inequalities in health • Canada has the ability to build on these experiences and aim to be the healthiest nation with the smallest gap in health • All Canadians have a role to play – individuals, communities, NGOs, governments and the private sector Source: Slide directly from PHAC Reference Deck
Canadian Medical Assoc. recommends HIA be conducted on broad federal policies May 2012, Canadian Medical Association (CMA), appearing before the House of Commons Standing Committee on Finance, re-iterated its concerns that policy-makers are not paying adequate attention to the social determinants of health, factors such as income, job security, housing, food security and other areas that have a major impact on health outcomes. CMA is calling on the federal government to adequately factor health concerns into policy development and decisions, recommending that “a health impact assessment be carried out ... on all cabinet decisions (to) take into account the possible impacts on health...” in order “to assess upstream the consequences of any policy on the health of Canadian, rather than try to fix it after the policy is in place”. Source: CMA Press Release http://www.digitaljournal.com/pr/734668
Health Equity Assessment Tool (HEAT)original: New Zealand Ministry of Health • What inequalities exist in relation to the health issue under consideration. • Who is most advantaged and how? • How did the inequalities occur? What are the mechanisms by which the inequalities were created, maintained or increased? • Where/ how will you intervene to tackle this issue? • How will you improve Maori health outcomes and reduce health inequalities experienced by Maori? • How could this intervention affect health inequalities? • Who will benefit most? • What might the unintended consequences be? • What will you do to make sure the intervention does reduce inequalities? • How will you know if inequalities have been reduced? Source: Signal L, Martin J, Cram F, Robson B. 2008. The Health Equity Assessment Tool: A user’s guide. Wellington: Ministry of Health. As accessed via http://www.pha.org.nz/documents/health-equity-assessment-tool-guide1.pdf 11
Modified HEAT used in H1N1 Responsemodified by: Manitoba Health, Equity & Ethics Planning Table • What inequalities exist in relation to the health issue under consideration? • What are the mechanisms by which the inequalities were created, maintained, or increased? • How could the proposed intervention affect health inequalities? Consider these questions for the following groups: • First Nations (on and off reserve) • Métis • Low income people or families; homeless people • People who are not fluent (oral and written) in English or French, • People with disabilities 12
Manitoba Health Office of the Chief Provincial Public Health Officer Health Equity Unit • Marcia Anderson DeCoteau, MD MPH FRCPC Medical Lead marcia.anderson@gov.mb.ca • Karen Serwonka, , BA MHSc Cert HIA Senior Policy Advisor karen.serwonka@gov.mb.ca Vision: All people in Manitoba have an equal opportunity to be healthy. Mission: to be a Centre of Excellence in leading the incorporation of health equity considerations into all aspects of program and policy development across government, including the development of a “health in all policies” approach that will impact the underlying social determinants of population health and health inequity. Mandate: to lead and/or collaborate on strategic initiatives and innovations that promote the equal opportunity for all Manitobans to be healthy. This includes, but is not limited to, acquiring and disseminating action-oriented knowledge and building capacity throughout the Provincial government to address the social determinants of health and advance health equity. 13