Download
1 / 55
820 likes | 1.55k Views
What’s New in HER2: Current Issues in HER2 Positive Breast Cancer. Kristine Abueg , RN, MSN, OCN®, CBCN ® Oncology Clinical Trials Kaiser Permanente, Roseville Coordinator, 2011-2103 Targeted and Biological Therapies Special Interest Group. Today in a Nutshell.

E N D
What’s New in HER2:Current Issues in HER2 Positive Breast Cancer Kristine Abueg, RN, MSN, OCN®, CBCN ® Oncology Clinical Trials Kaiser Permanente, Roseville Coordinator, 2011-2103 Targeted and Biological TherapiesSpecial Interest Group
Today in a Nutshell • ErbB tyrosine kinase family receptor alterations drive HER2+ breast cancer. • HER2+ mutation associated with poor outcomes. • Trastuzumab offers significant clinical benefit. • Current Challenges in HER2 breast cancer • Effective Identification of appropriate populations • Overcoming trastuzumab resistance and recurrence • Trastuzumab resistance and recurrence associated with alternative signaling pathways • New agents in development target alternative signaling pathways
Part I Her2 biology….as we currently understand it
The Human Epidermal Growth Factor Receptor (HER) family of cell surface receptors [ErbB = HER2] HER1/ EGFR HER 2 HER 3 HER4 Extracellular ( Receptor) Transmembrane Domain Intracellular Kinase RH Gunby et al. Oncogenic Fusion Tyrosine Kinases As Molecular Targets for Anti-Cancer Therapy. Anti-Cancer Agents in Medicinal Chemistry, 2007; 7:594-611. Images created by Kristine Abueg.
Receptor Activation via two dimer formations.HER2 is the preferred dimer partner • Heterodimerization HER 2 HER 2 HER 2 HER 3 Homodimerization P P PI3K RAS Cell Signal Cascade mTOR Raf Angiognesis Proliferation ↓ Apoptosis ↑Survival Rowinsky. Oncologist. 2003;8(suppl 3):5-17. Yarden et al. Nature Rev Mol Cell Biol. 2001;2:127-137. Images created by Kristine Abueg
HER2 partnering results in the strongest signal HER1:HER3 HER1:HER2 HER1:HER4 HER4:HER4 HER3:HER3 HER2:HER3 HER2:HER2 HER2:HER4 HER1:HER1 HER3:HER4 + + + + + + + + + + + + + + + Signaling activity Tzahar et al. Mol Cell Biol. 1996;16:5276-5287. Lenferink et al. EMBO J. 1998;17:3385-3397.
HER2-positive clinical impact • Associated with poor outcomes: • ↑ Distant metastases • ↑ Nodes + disease • ↑ Highest risk of recurrence • ↓Overall Survival • High grade tumors • Endocrine therapy resistance • “Trastuzumab [and other HER2 targeted therapies] have changed the course of HER2 positive breast cancer (Mukohara, 2011)”
Trastuzumab ‘s Dual-Kill Mechanism Immune Cells Immune Cells • Antibody Dependent Cellular Toxicity (ADCC) • Attached trastuzumab signals immune destruction • Prevents Intracellular Cell Signaling • Induces Apoptosis • Prevents Proliferation Trastuzumab HER2 Cell Signaling Activation Apoptosis Images created by Kristine Abueg
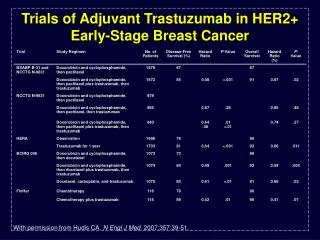
Pivotal Trastuzumab trials: Adjuvant A: Doxorubicin (Adriamycin); C: Cylclophosphamide; T: Paclitaxel (Taxol); H: Herceptin (Trastuzumab) PFS: Progression Free Survival, OS: Overall Survival
Pivotal Trastuzumab trials: Adjuvant A: Doxorubicin (Adriamycin); C: Cylclophosphamide; T: Paclitaxel (Taxol); H: Herceptin (Trastuzumab) PFS: Progression Free Survival, OS: Overall Survival
Pivotal Trastuzumab trials: Metastatic Cobleigh MA, Vogel CL, Tripathy D, et al. Multinational study of the efficacy and safety of humanized anti-HER2 monoclonal antibody in women who have HER2-overexpressing metastatic breast cancer that has progressed after chemotherapy for metastatic disease. J ClinOncol. 1999;17:2639-2648.
Pivotal Trastuzumab trials: Metastatic Cobleigh MA, Vogel CL, Tripathy D, et al. Multinational study of the efficacy and safety of humanized anti-HER2 monoclonal antibody in women who have HER2-overexpressing metastatic breast cancer that has progressed after chemotherapy for metastatic disease. J ClinOncol. 1999;17:2639-2648.
Pivotal Trastuzumab trials: Metastatic Cobleigh MA, Vogel CL, Tripathy D, et al. Multinational study of the efficacy and safety of humanized anti-HER2 monoclonal antibody in women who have HER2-overexpressing metastatic breast cancer that has progressed after chemotherapy for metastatic disease. J ClinOncol. 1999;17:2639-2648.
Paradigm shift • “Clearly, the results reported in this issue of the Journal are not evolutionary but revolutionary. The rational development of molecularly targeted therapies points the direction toward continued improvement in breast cancer therapy. Other targets and other agents will follow. However, trastuzumab and the two reports in this issue will completely alter our approach to the treatment of breast cancer” Gabe Hortobayi, NEJM, 2005
Trastuzumab Side Effect Profilewww.herceptin.com • Cardiomyopathy • Baseline and q3 mos LVEF (should be >50%) • S/S congestive heart failure • Pulmonary Toxicity • Dyspnea, interstitial pneumonia, ARDS • Neutropenia exacerbation • Infusion reaction (cytokine release syndrome) • GI: diarrhea, stomatitis • Risk to pregnancy
Trastuzumab: Key Patient Education Schedule: • Weekly: Loading dose 4mg/kg over 90 min followed by 2mg/kg over 30 min • Q3 week: Loading dose 8mg/kg over 90 followed by 6 mg/kg over 30 min
Trastuzumab regimens: Adjuvant AC→TH: Total regimen lasts 64 weeks • AC: Four cycles of Adriamycin® (doxorubicin) and Cytoxan® (cyclophosphamide) chemotherapy given every 3 weeks; followed by • TH: Twelve cycles of Herceptin given weekly, along with 4 cycles of Taxotere® (docetaxel) given every 3 weeks OR 4 cycles of Taxol® (paclitaxel) given every 3 weeks OR 12 cycles of paclitaxel given weekly; followed by • Fourteen cycles of Herceptin administered alone every 3 weeks to complete 52 total weeks (1 year) of Herceptin therapy TCH: Total regimen lasts 52 weeks • TCH: Six cycles of Taxotere and Paraplatin® (carboplatin) chemotherapy given every 3 weeks, along with 18 cycles of Herceptin given weekly; followed by • Twelve cycles of Herceptin given every 3 weeks to complete 52 total weeks (1 year) of Herceptin therapy Herceptin monotherapy: Regimen lasts 52 weeks • Eighteen cycles of Herceptin administered every 3 weeks for 52 total weeks (1 year) of Herceptin therapy • Herceptin is administered alone after receiving a full course of chemotherapy
Trastuzumab regimens: Metastatic • Herceptin is administered alone or in combination with Taxol at an initial dose of 4 mg/kg • Subsequent doses of 2 mg/kg given once weekly until disease progression or unacceptable toxicity occurs
7 Trastuzumab has offered significant benefit to our HEr2+ breast cancer population, however there is still some work to be done.
Identifying appropriate patients • Resistance
Challenge #1: Identification of appropriate populations Objectives: • Discuss current ASCO/NCCN guidelines for HER2 testing. • Discuss current controversies in HER2 testing • Accuracy • Predictive value • Implications for patients and oncology professionals
Invasive Breast Cancer Specimen Immunohistochemistry (IHC) Subjective “scoring” of HER2 surface protein expression IHC 1+ IHC 0+ HER2 Negative IHC 1+ HER2 Negative IHC 2+ Equivocal IHC 3+ Positive Anti-HER2 therapy In-Situ Hybridization (-ISH) “Quantitative” ratio of HER2 to normal genes (CEP17) HER2/ CEP17 > 2.0 FISH positive = HER2+ HER2 gene amplification HER2/ CEP17 ≤ 2.0 FISH neg = HER2- No HER2 gene amplification Paik, et al (2002). Anti-HER2 therapy
Testing Issue #1 How accurate are IHC and -ISH scoring? • Provocative Date leading to Re-examination of current practice patterns. Community Pathology Lab Breast Specimen “Reference” Pathology Lab
Clinical Implications • Validation of community labs • More stringent revision of ASCO/CAP guidelines Comparison of ASCO revisions Her 2 targeted Tx Old guideline -ISH Negative < 2.0 -ISH Positive ≥ 2.0 New guideline -ISH - < 1.8 -ISH + ≥ 2.2 Equivocal 1.8-2.2 Retest Her 2 targeted Tx Wolff (2007); Raji (2007)
Testing Issue #2 How predictive areIHC and -ISH scoring?HER2 neg patients still benefited from trastuzumab. Community Pathology Lab Breast Specimen HER2- HER2+ “Reference” Pathology Lab Paik, 2007
Clinical Implication:Expansion of HER2 “sensitive” definition? • 2010 ASCO, Collins : Effect of trastuzumab on antibody-dependent cellular cytotoxicity (ADCC) in HER2 nonamplified (non-amp) breast cancer (BC) cells. • Demonstrated cell toxicity even when HER2 – • Clinical trials on going: • trastuzumab in the IHC 1+ • Trastuzumab in FISH negative • Possible expansion of trastuzumab application • Possible revision of HER2 positive criteria Wolff (2007); Raji (2007)
Despite trastuzumab’s significant survival benefit, a large proportion of HER-2 positive breast cancer will develop resistance, and ultimately recurrence and progression. The key to understanding - and ultimately mitigating- this resistance lies in the HER2 signaling pathway.
Resistance to trastuzumab: Proposed mechanisms Trastuzumab • Sterichinderance (something getting in the way) • Alternate signaling from other HER family member • Alternate signaling from non-HER receptors • Altered intracellular signaling “other” HER2 HER3 P P P Cell Signaling Activation Images created by Kristine Abueg
PART 2: New Anti-HER2 Agents Objectives: • Review of lapatinib mechanism, efficacy, side effects, and patient management. • Investigational Agents • Rationale for mechanism • Published data & on-going trials • Implications for patients and oncology professionals
Anti-HER 2 Agents HER1/ EGFR HER 2 HER 3 Trastuzumab TDM-1 Pertuzumab Neratinib Lapatinib Lapatinib Everolimus RH Gunby et al. Oncogenic Fusion Tyrosine Kinases As Molecular Targets for Anti-Cancer Therapy. Anti-Cancer Agents in Medicinal Chemistry, 2007; 7:594-611. Images created by Kristine Abueg.
Lapatinib Efficacy in Trastuzumab Resistant Disease • Trastuzumab “cleaves” extracellular domain of HER2 • p95HER2 stimulates intracellular cell signaling • Trastuzumab ineffective • Lapatinib inhibits intracellular cell signaling Post- trastuzumab HER2 Trastuzumab p95HER2 Lapatinib Lapatinib Cell Signaling Activation Scaltriti, et al 2007; Mukohara 2011 Images created by Kristine Abueg
Lapatinib demonstrates prolonged progression free survival after trastuzumab failure FDA Approved Indications: Lapatinib in Metastatic HER2+Disease Johnston et al 2009, Schwartzerg, et al 2010. Geyer, et al 2006 Cameron, et al 2008.
LapatinibWITHTrastuzumab(Prior to Trastuzumab Resistance) Trastuzumabmonotherapy Trastuzumuab + Lapatinib combination Trastuzumab Trastuzumab Lapatinib Lapatinib Cell Signaling Activation Cell Signaling Activation Scaltriti, et al 2007; Mukohara 2011 Images created by Kristine Abueg
What is Lapatinib’s benefit prior to trastuzumab failure? Ongoing Adjuvant Trials Altto Adjuvant Lapatinib and/or Trastuzumab Treatment Optimisation Trial Options: Concurrent taxane chemotherapy Closed to “non-inferiority threshold” Ongoing data analysis Combined targeting Adjuvant Lapatinib and/or Trastuzumab Treatment Optimisation Trial www.alttotrials.com; http://www.breastinternationalgroup.org
Lapatinib efficacy prior to trastuzumab failure? Lapatinib: Ongoing NEOAdjuvant Trials NEOAltto NEOAdjuvant Lapatinib and/or Trastuzumab Treatment Optimisation Trial Surgery Pathological Complete Response 24.7% 29.5% 51.3% 23% 2% 21% Diarrhea Neutropenia Skin 16% 3% 9% 7% 3% 7% No significant cardiac toxicity in either arm Baselga, 2010
Lapatinib: Key Patient EducationDosing Instructions • Empty Stomach: 1 hr before; 2 hrs after food • Take all at once (do not divide daily dose) • Metastatic with capecitabine: 1250 mg d1-d21 • Metastatic with letrozole: 1500 mg qD Lapatinib 1250 mg qD d1-d21 Capecitabine 1500 mg/m2 BID d1-d14 Lapatinib 1500 mg qD continuously Letrozole 2.5 mg qD continuously Lapatinib Package Insert
Lapatinib: Key Patient EducationInteractions CYP3A4 inducers CYP3A4 inhibitors INCREASE Lapatinib concentration. INCREASED Toxicity Grapefruit Cimetidine Amiodarone Cyclosporines Itraconazole Ketaconazoles Omeprazole Clarithromycin DECREASE Lapatinib concentration. DECREASED Efficacy • Alprazolam • Buspirone • Ca+ channel blockers • Dexamethasone • Erythromycine • Fentanyl • Simvastatine • St. John’s Wort http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1312247/table/TU1/
Lapatinib: Key Patient EducationCommonSide Effects Recommend Frankel & Palmieri, 2010 CJON 14(2). • Gastrointestinal : Diarrhea (>20%) • Generally mild • Baseline and ongoing assessment • BRAT diet; hydration • Loperamide (grade 2) and oncreotide (grade 3 or persistent) • Dermatological: Rash (>50%) • Maculopapular or papulopustular rash • No documented correlation between severity and efficacy • Moisturize & Protect • Coverage >50% body surface or symptomatic – hold lapatinib, topical corticosteroids and oral tetracyclines Crown, et al 2009; Frankel and Palmieri 2010.
Lapatinib: Lab Monitoring • Hepatic Parameters • AST or ALT > 3x Upper Limit of Normal • Total Bilirubin > 2x Upper Limit of Normal • Cardiac Dysfunction • EKG changes: QT prolongation >480mSec • MUGA/ECHO changes: Ejection Fraction↓ but lower than with trastuzumab
Neratinib: Efficacy in Trastuzumab Resistant Disease • Similar mechanism to lapatinib: • Trastuzumab “cleaves” extracellular domain of HER2 • p95HER2 stimulates intracellular cell signaling • Trastuzumab ineffective • Neratinib blocks ErbB1, ErbB2, and ErbB4 & inhibits intracellular cell signaling Post- trastuzumab HER2 ErbB1 Trastuzumab p95HER2 Neratinib Neratinib Cell Signaling Activation Scaltriti, et al 2007; Mukohara 2011 Images created by Kristine Abueg
Does Neratinib offer a benefit in metastatic breast cancer? Response Rate 24% 26% 16 week PFS 59% 78% 23% 40% 40 week PFS Diarrhea (mild) 85% Nausea, fatigue, acneuform rash Burstein, 2009
Everolimus : Efficacy in Trastuzumab Resistant Disease • Everolimus = mTOR inhibitor • Early Phase I/II data • mTOR + Trastuzumab Post- trastuzumab HER2 Trastuzumab p95HER2 Everoliumus Everoliumus Cell Signaling Activation Marrow, et al (2011) Images created by Kristine Abueg
Antibody Drug Conjugate:TDM-1 (trastuzumab emtansine) Immune Cells • Trastuzumab bound to cytotoxic chemotherapy • Retains trastuzumab ADCC action • Targeted chemotherapy delivery to cell DM1 Immune Cells Trastuzumab Intracellular Chemo Delivery Apoptosis Images created by Kristine Abueg Juntilla, 2010, Lewis, 2011,Scaltriti, et al 2007; Mukohara 2011
TDM-1 efficacy, tolerability, and safety TDM4450g First line HER2 metastatic Median Duration of Response Overall Response 9.5 months Not yet reached 58% 64% Hurvitz, et al Abstr 5001, ESMO, 2011. Perez, et al, Abstr LBA 3. ESMO, 2010
TDM-1 on-going clinical trials • 2010 FDA submission for accelerate approval denied pending Phase III data completion • 2nd line, Phase III (EMILIA) [closed to accrual] • TDM 1 vs. Capecitabine and Lapatinib • 1st line, Phase II (MARIANNE) [closed to accrual] • TDM1/Pertuzumab vs. TDM1 vs. Docetaxel/Trastuzumab • 3rd line, Phase II (THERESA) [pending] • TDM vs. Physician’s Choice
Heterodimerization Targeting:Pertuzumab (Omnitarg ®) THREE ACTIONS • Blocks HER2/HER1 and HER2/HER3 dimerization • Binds at separate site from trastuzumab. Synergistic effect. • Stimulates antibody-dependent cell-mediated cytotoxicity ADCC Trastuzumab Pertuzumab Pertuzumab Apoptosis Scaltriti, et al 2007; Mukohara 2011 Images created by Kristine Abueg
Among all possible dimers, the HER2:HER3 pair has the strongest mitogenic signaling HER1:HER3 HER1:HER2 HER1:HER4 HER4:HER4 HER3:HER3 HER2:HER3 HER2:HER2 HER2:HER4 HER1:HER1 HER3:HER4 + + + + + + + + + + + + + + + Signaling activity Tzahar et al. Mol Cell Biol. 1996;16:5276-5287. Lenferink et al. EMBO J. 1998;17:3385-3397.
Pertuzumab efficacy in the metastatic setting CLEOPATRA data Baselga, 2012, Lenihan, 2011. Progression Free Survival
Pertuzumab efficacy in the metastatic setting CLEOPATRA data Baselga, 2012, Lenihan, 2011. 46.3% 66% Diarrhea Neutropenia Skin 7.6 % 13.8% 24.2 % 33.7% No notable increase in cardiac effects. No notable increase in infusion reactions. Most AE’s were grade 1-2 (ie mild)