Download
1 / 41
520 likes | 2.54k Views
Infection control, hospital infections

E N D
Infection control Dr.T.V.Rao MD Professor of Microbiology Dr.T.V.Rao MD
A Tribute to Ignaz Semmelweiss (1818-1865) Ignaz Semmelweiss (1818-1865) • Obstetrician, practised in Vienna • Studied puerperal (childbed) fever • Established that high maternal mortality was due to failure of doctors to wash hands after post-mortems • Reduced maternal mortality by 90% • Ignored and ridiculed by colleagues Dr.T.V.Rao MD
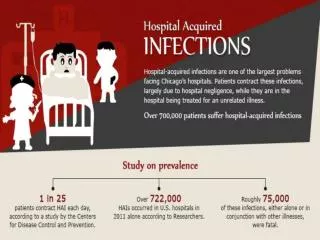
Hospital Infections are Emerging challenges in Health Care • Hospital-associated infections represent a serious and growing health problem. The Centers for Disease Control and Prevention (CDC) estimates that 2 million people acquire hospital-associated infections each year and that 90 000 of these patients die as a result of their infections. A variety of hospital-based strategies aimed at preventing such infections have been proposed. Dr.T.V.Rao MD
What is Infection Control • Infection controlis the discipline concerned with preventing nosocomial or healthcare-associated infection. As such, it is a practical (rather than an academic) sub-discipline of epidemiology. It is an essential (though often under-recognized and under-supported) part of the infrastructure of health care. Infection control and hospital epidemiology are akin to public health practice, practiced within the confines of a particular health-care delivery system rather than directed at society as a whole. Dr.T.V.Rao MD
Beginning of Hospital Infection Programme • Modernhospital infection control programs first began in the 1950s in England, where the primary focus of these programs was to prevent and control hospital-acquired staphylococcal outbreaks. In 1968, the American Hospital Association published "Infection Control in the Hospital," the first and only standards available for many years. Dr.T.V.Rao MD
Beginning of Accreditation • In 1969, the Joint Commission for Accreditation of Hospitals--later to become the Joint Commission on Accreditation of Healthcare Organizations (JCAHO)--first required hospitals to have organized infection control committees and isolation facilities. Dr.T.V.Rao MD
CDCInitiates Hospital Infection Branch • In 1972, the Hospital Infections Branch at the CDC was formed and the Association for Practitioners in Infection Control was organized. By the close of the decade, the first CDC guidelines were written to answer frequently asked questions and establish consistent practice. Dr.T.V.Rao MD
Infection Control Challenges of Healthcare in 2000 • Decreasing reimbursement • Increasing emerging infections • Increasing resistant organisms • Increasing drug costs • Institute of Medicine Report--healthcare-associated infections • Nursing shortage • OSHA safety legislation • Multiple benchmark systems • FDA legislation on reuse of single-use devices Dr.T.V.Rao MD
Why Everyone Concerned with Hospital Infections • The Centers for Disease Control (CDC) estimates that 2 million U.S. patients a year acquire hospital-related infections. These infections cost an average of $47,000 per patient to treat and cause 90,000 deaths each year. The added cost to hospitals is $4.8 billion annually in extended care and treatment. Dr.T.V.Rao MD
Developing Infection Control Programme • Every infection control program should develop a well-defined written plan outlining the organizational philosophy regarding infection prevention and control. The plan should take into account the goals, mission statement, and an assessment of the infection control program. It should include a statement of authority, and should review patient demographics including geographic locations of patients served by the healthcare system Dr.T.V.Rao MD
Surveillance • The surveillance is the cornerstone of the infection control practice because it allows to identify the areas where the outcomes are below expectations and we can improve. • Examples of centrally driven surveillance include MRSA bacteraemia surveillance Dr.T.V.Rao MD
Defining as precisely as possible the event to be surveyed (case definition) Collecting the relevant data in a systematic, valid way Consolidating the data into meaningful arrangements Analyzing and interpreting the data Using the information to bring about change Key elements of surveillance adapted from R. Haley Dr.T.V.Rao MD
Surveillance • The key to ongoing monitoring is surveillance for nosocomial infections. Various techniques for surveillance have been described and evaluated including total house surveillance, targeted surveillance, Kardex, or laboratory-base Dr.T.V.Rao MD
Surveillance for nosocomial infection Patterns of transmission of nosocomial infections Outbreak investigation Isolation precautions Evaluation of exposures Employee health Disinfection and sterilization Hospital engineering and environment water supply air filtration Reviewing policies and procedures for patient care Areas of interest to a healthcare epidemiologist Dr.T.V.Rao MD
Educational Psychology • Most difficult part of infection control practioners is overcome the reluctance of humans to change their behaviour • Every one knows importance of hand hygiene and sterile technique • However hand hygiene compliance is poor among health care workers and even after intensive education and improved marginally Dr.T.V.Rao MD
Staff Training in ICP • Education programs for employees and volunteers are one method to ensure competent infection control practices. It is a unique challenge since employees represent a wide range of expertise and educational background. The ICP must become knowledgeable in adult education principles and use educational tools and techniques that will motivate and sustain behavioral change. Dr.T.V.Rao MD
Requires cooperation, understanding and support of hospital administration and medical/surgical/nursing leadership There is no simple formula: Every facility is different Every facility’s problems are different Every facility’s personnel are different The facility must develop its own unique program Organizing for Infection Control Dr.T.V.Rao MD
Document Antibiograms with WHONET • WHONET is a free Windows-based database software developed for the management and analysis of microbiology laboratory data with a special focus on the analysis of antimicrobial susceptibility test results. Dr.T.V.Rao MD
Antibiotic Stewardship • It carries considerable interest in implementing and monitoring interventions to optimize prescribing of antimicrobial drugs Dr.T.V.Rao MD
Can we change the Situation? • Antibiotic policies may be introduced primarily to reduce total Antibiotic use to reduce in appropriate prescribing • Many using the most broad spectrum drugs in the first line ? Dr.T.V.Rao MD
Use of Antibiotic Policies • It has been estimated that up to 50 % of the antimicrobial prescribing is inappropriate in terms of choice, duration and indication of treatment. • The coordination of clinician and microbiologist to reduce in implementation of antibiotic guidelines carries a higher importance. Dr.T.V.Rao MD
Alert Microbes • Hospital acquired alert organisms generally those organisms that have resistance to a range of antibiotics and are capable of spreading • Methicillin resistant Staphylococcus aureus • Gram negative bacilli resistant to gentamicin, extended spectrum beta lactamases • Vancomycin resistant Enterococci Dr.T.V.Rao MD
All Isolates • All positive isolates clinical isolates from high risk areas Intensive care areas Intensive care areas special care baby units • Positive clinical isolates from sites of interest to infection control team ( catheter related infections, • Urinary and Intravascular operative samples • Removed prosthesis, heart valves , artificial joints. Dr.T.V.Rao MD
ESKAPE - Bacteria • ESKAPE bacteria— Enterococcus faecium, Staphylococcus aureus, Klebsiella species, Acinetobacter baumannii, Pseudomonas aeruginosa, and Enterobacter species—are among the biggest threat of infectious diseases physicians face today, Dr.T.V.Rao MD
ESKAPE Bacteria are Major Nosocomial Agents • According to the latest data from the Centers for Disease Control and Prevention (CDC), the six ESKAPE bacteria are responsible for two thirds of all health care-associated infections (HAIs). Dr.T.V.Rao MD
What is best for Hand Hygiene • A single application of 60 – 70 % Ethanol or Isopropanol with emolument and with or with out antiseptic like • 1 Chlorhexidine • 2 Povidone –iodine • Triclosan • Proved to be more effective than soap and water Dr.T.V.Rao MD
How you rub your hands • A volume of 3 ml is pored into cupped hands and rubbed to dryness Dr.T.V.Rao MD
If your hands are soiled • Do not forget to a preliminary wash with soap or detergent and water is required before the application of Alcoholic solution Dr.T.V.Rao MD
Why we need Computers • The use of technology rather than manual system should enable data to be Analysed more easily and encouraged. • So many soft wares in market • But should be compatible with clinical laboratory system and integrate with hospital information technology patient management system in order to obtain with meaningful data with minimal effort. Dr.T.V.Rao MD
Infection Control Programme and Documentation • Goals of the infection control program need to be incorporated into the mission statement of the facility. A mission statement should tell who you are, what you do, and should communicate a clear view of purpose and set a strategy for accomplishing the goal Dr.T.V.Rao MD
Good House Keeping a Boon to Infection Control Dr.T.V.Rao MD
Break the Chain of Infections • 1. Organisms that can cause infection are subject to risk assessment under the COSHH regulations and Management of Health and Safety at Work Regulation 1992. Dr.T.V.Rao MD
The Infection Control Team • Consist of at least an infection control practitioner who should be trained for the purpose; carry out the surveillance programme; develop and disseminate infection control policies; monitor and manage critical incidents; coordinate and conduct training activities. Dr.T.V.Rao MD
Involvement of Physicians More Important Physicians to be more involved and lead quality improvement efforts in their respective healthcare settings. Drs. Pronovost and Marsteller suggest that even though quality improvement efforts exist, there is not enough data supporting the notion that quality improvement efforts are actually enhancing patient outcomes. One of the reasons for this lack of progress, they say, is inadequate physician engagement and leadership in quality improvement work. Peter Pronovost, MD, PhD, and Jill Marsteller, PhD, MP Dr.T.V.Rao MD
Major Responsibilities of I C P • The major responsibilities for ICPs to oversee include surveillance, specific environmental monitoring, continuous quality improvement, consultation, committee involvement, outbreak and isolation management, regulatory compliance and education. To plan, coordinate, and succeed in fulfilling these responsibilities, many ICPs have to redefine their roles. More ICPs are becoming managers by creating multidisciplinary support teams to carry out many of the functions. Dr.T.V.Rao MD
Involvement of Physicians More Important Physicians to be more involved and lead quality improvement efforts in their respective healthcare settings. Drs. Pronovost and Marsteller suggest that even though quality improvement efforts exist, there is not enough data supporting the notion that quality improvement efforts are actually enhancing patient outcomes. One of the reasons for this lack of progress, they say, is inadequate physician engagement and leadership in quality improvement work. Peter Pronovost, MD, PhD, and Jill Marsteller, PhD, MP Dr.T.V.Rao MD
GUIDELINES AND RECOMMENDATIONS • Hand washing and Hospital Environmental Control * Immunization * Infectious Diseases Control * Intravascular Device-Related Infections and its control * Isolation Precautions Dr.T.V.Rao MD
Scientific Documentation Reduces Hospital Infections • Researchers evaluated the effect of an electronic medical record on the use of antimicrobial agents and infection rates of Clostridium difficile and MRSA. Results showed that implementation of an EMR significantly increased chart reviews and antimicrobial recommendations, leading to a decrease in antimicrobial use and MRSA as well as C. difficile infection rates. Dr.T.V.Rao MD
A saying applies to all activities including hospital surveillance • If you are not measuring it, you are not managing it. Dr.T.V.Rao MD
Programme Created by Dr.T.V.Rao MD for Health awareness on Hospital acquired Infections • Email • doctortvrao@gmail.com Dr.T.V.Rao MD