Download
1 / 33

E N D
Cytomegalovirus Dr.T.V.Rao MD Dr.T.V.Rao MD
Cytomegalovirus infections • Ubiquitous virus most populations -infections in early childhood often asymptomatic • Latency • Clinical disease increasing due to increasing number of immunocompromised patients Dr.T.V.Rao MD
Properties • Belong to the betaherpesvirus subfamily of herpesvirusesdouble stranded DNA enveloped virus • Nucleocapsid 105nm in diameter, 162 capsomers • The structure of the genome of CMV is similar to other herpesviruses, consisting of long and short segments which may be orientated in either direction, giving a total of 4 isomers. • A large no. of proteins are encoded for, the precise number is unknown. Dr.T.V.Rao MD
Virus StructureEnveloped, slightly pleomorphic Spherical 120 – 200 nm in diameter CapsidEnvelopeTegumentGenomedouble stranded DNA per virion Dr.T.V.Rao MD
Why are herpes viruses (and especially CMV) so fascinating from an evolutionary standpoint? They are ancient Latency = highly evolved While many viruses deal with evolution “passively” (i.e. mutate), herpes viruses “actively” target mechanisms Dr.T.V.Rao MD
Virion: Spherical, enveloped, 150-200 nm in diameter Genome: Double-stranded DNA, linear, 240 kbp, reiterated sequences Proteins: only a few have been characterized Replication: Nucleus, bud from nuclear membrane Virus classification: Group I: ds DNA; Family: Herpesviridae; Genus: Cytomegalovirus; Species: Human herpesvirus 5 (HHV-5) Virology Dr.T.V.Rao MD
Human Cytomegalovirus A complex -herpesvirus Large genome (230kb) Slow replicating Restricted host range Infects 60-90% of the population worldwide, typically asymptomatic infection Infection in immunocompromised individuals life threatening Stem cell and solid organ transplant recipients HIV infected individuals Cancer patients receiving intensive chemotherapy regimens Infection in utero: Leading cause of infectious disease related birth defects 1 in 100 infected; 1 in 1000 present symptoms/pathology Mild to severe hearing loss Cognitive deficits Physical abnormalities Dr.T.V.Rao MD
Human Cytomegalovirus Virion Structure envelope glycoproteins tegument capsid DNA core 200 nm Dr.T.V.Rao MD
How is CMV Spread? • Person to person contact (kissing, sexual contact, getting saliva or urine on hands and then touching eyes, or the inside of nose or mouth) • Through the breast milk of an infected woman • Infected pregnant women can pass the virus to their unborn babies • Blood transfusions and organ transplantations Dr.T.V.Rao MD
Pathogenesis • Once infected, the virus remains in the person for life and my be reactivated from time to time, especially in immunocompromised individuals. • The virus may be transmitted in utero, perinatally, or postnatally. Perinatal transmission occurs. • Perinatal infection is acquired mainly through infected genital secretions, or breast milk. Overall, 2 - 10% of infants are infected by the age of 6 months worldwide. Perinatal infection is thought to be 10 times more common than congenital infection. • Postnatal infection mainly occurs through saliva. Sexual transmission may occur as well as through blood and blood products and transplanted organ. Dr.T.V.Rao MD
Clinical Manifestations • Congenital infection - may result in cytomegalic inclusion disease • Perinatal infection - usually asymptomatic • Postnatal infection - usually asymptomatic. However, in a minority of cases, the syndrome of infectious mononucleosis may develop which consists of fever, lymphadenopathy, and splenomegaly. The heterophil antibody test is negative although atypical lymphocytes may be found in the blood. • Immunocompromised patients such as transplant recipients and AIDS patients are prone to severe CMV disease such as pneumonitis, retinitis, colitis, and encephalopathy. • Reactivation or reinfection with CMV is usually asymptomatic except in immunocompromised patients. Dr.T.V.Rao MD
Fetus transmission from mother via placenta clinically normal 80% causes congenital CMV death 1% Cytomegalic inclusion disease % late onset hearing defect / mental retardardation 15% Infant transmission during birth or breast feeding usually asymptomatic Cytomegalovirus infections Dr.T.V.Rao MD
Pregnant Women and CMV • Contact with the saliva or urine of young children is a major cause of CMV infection among pregnant women. • Risk of CMV infection is likely to be reduced by careful attention to good personal hygiene, such as hand washing. Dr.T.V.Rao MD
Congenital Infection • Defined as the isolation of CMV from the saliva or urine within 3 weeks of birth. • Commonest congenital viral infection, affects 0.3 - 1% of all live births. The second most common cause of mental handicap after Down's syndrome and is responsible for more cases of congenital damage than rubella. • Transmission to the fetus may occur following primary or recurrent CMV infection. 40% chance of transmission to the fetus following a primary infection. • May be transmitted to the fetes during all stages of pregnancy. • No evidence of teratogenicity, damage to the fetus results from destruction of target cells once they are formed. Dr.T.V.Rao MD
Symptoms of Congenital CMV Temporary SymptomsLiver problemsSpleen problemsJaundice (yellow skin and eyes)Purple skin splotchesLung problemsSmall size at birthSeizuresPermanent Symptoms or DisabilitiesHearing lossVision lossMental disabilitySmall headLack of coordinationSeizuresDeath Dr.T.V.Rao MD
Cytomegalic Inclusion Disease • CNS abnormalities - microcephaly, mental retardation, spasticity, epilepsy, periventricular calcification. • Eye - choroidoretinitis and optic atrophy • Ear - sensorineural deafness • Liver - hepatosplenomegaly and jaundice which is due to hepatitis. • Lung - pneumonitis • Heart - myocarditis • Thrombocytopenic purpura, Haemolytic anaemia • Late sequelae in individuals asymptomatic at birth - hearing defects and reduced intelligence. Dr.T.V.Rao MD
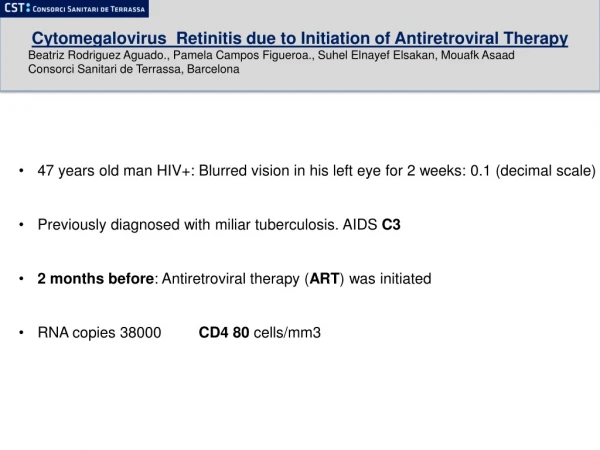
CMV Retinitis small floaters foggy or blurred vision loss of central or peripheral vision routine exam when the infectious process is early and located in the peripheral retina loss of vision retinal detachment Dr.T.V.Rao MD
CMV retinitis Dr.T.V.Rao MD
CMV retinitis Dr.T.V.Rao MD
Diagnosis presence of virus or antibody to CMV does not indicate that current disease is due to CMV Different strategies used in different clinical situations isolation of virus from urine within 30 days of birth * antigen detection in buffy coat - indicates viraemia Cytomegalovirus infections DIFFICULT Congenital CMV immunocompromised patient • * CMV specific Ig G positive indicates past infection Dr.T.V.Rao MD
Laboratory Diagnosis • Direct detection • biopsy specimens may be examined histologically for CMV inclusion antibodies or for the presence of CMV antigens. However, the sensitivity may be low. • The pp65 CMV antigenemia test is now routinely used for the rapid diagnosis of CMV infection in immunocompromised patients. • PCR for CMV-DNA is used in some centers but there may be problems with interpretation. Dr.T.V.Rao MD
Laboratory Diagnosis • Virus Isolation • conventional cell culture is regarded as gold standard but requires up to 4 weeks for result. • More useful are rapid culture methods such as the DEAFF test which can provide a result in 24-48 hours. • Serology • the presence of CMV IgG antibody indicates past infection. • The detection of IgM is indicative of primary infection although it may also be found in immunocompromised patients with reactivation. Dr.T.V.Rao MD
Serologic testing Paired antibody titers (4-fold increase in convalescent phase compared to acute phase) ELISA to determine if acute infection, prior infection, or passively acquired maternal antibody in an infant is present. CMV IgM titers for congenital infection Other tests include CF test, fluorescence assays (CMV pp65 antigenemia test, IFA, ACIF), indirect haemagglutination & PCR CMV should be suspected if a patient has symptoms of infectious mononucleosis but has negative test results for mononucleosis and Epstein-Barr virus, or if they show signs of hepatitis, but has negative test results for hepatitis A, B, and C. Laboratory Diagnosis Dr.T.V.Rao MD
PCR is more sensitive than shell vial or antigenemia assays Some patients may be pre-emptively treated unnecessarily using PCR strategies Quantitative PCR may be more sensitive than qualitative PCR No criteria for standard treatment threshold exist for quantitative CMV PCR PCR Based Screening Methods Dr.T.V.Rao MD
Treatment • Congenital infections - it is not usually possible to detect congenital infection unless the mother has symptoms of primary infection. If so, then the mother should be told of the chances of her baby having cytomegalic inclusion disease and perhaps offered the choice of an abortion. • Perinatal and postnatal infection - it is usually not necessary to treat such patients. • Immunocompromised patients - it is necessary to make a diagnosis of CMV infection early and give prompt antiviral therapy. Anti-CMV agents in current use are ganciclovir, forscarnet, and cidofovir. Dr.T.V.Rao MD
Prevention • No licensed vaccine is available. There is a candidate live attenuated vaccine known as the Towne strain but there are concerns about administering a live vaccine which could become latent and reactivates. • Prevention of CMV disease in transplant recipients is a very complicated subject and varies from center to center. It may include the following measures. • Screening and matching the CMV status of the donor and recipient • Use of CMV negative blood for transfusions • Administration of CMV immunoglobulin to seronegative recipients prior to transplant • Give antiviral agents such as acyclovir and Ganciclovir prophylactically. Dr.T.V.Rao MD
Reduce Chances of Contracting CMV • Wash hands often with soap and water for 15-20 seconds, especially after wiping runny noses, changing diapers, picking up toys, etc. If soap and water are not available, use alcohol-based hand gel. • Use soap and water or a disinfectant to clean hard surfaces that have been contaminated by secretions • Don’t share food, drinks, or eating utensils with young children • Don’t kiss young children on the lips—give them a big hug and a kiss on top of the head. • If you work in a day care center, limit close contact with children younger than 2½ years of age, especially if you've never been infected with CMV or don't know if you've been infected. Dr.T.V.Rao MD
CDC Stats: www.cdc.gov/cmv • Every hour, congenital CMV causes one child to become disabled • Each year, about 30,000 children are born with congenital CMV infection • About 8,000 children each year suffer permanent disabilities caused by CMV • About 1 in 150 children is born with congenital CMV infection • About 1 in 750 children is born with or develops permanent disabilities due to CMV Dr.T.V.Rao MD
Epidemiology • CMV is one of the most successful human pathogens, it can be transmitted vertically or horizontally usually with little effect on the host. • Transmission may occur in utero, perinatally or postnatally. Once infected, the person carries the virus for life which may be activated from time to time, during which infectious virions appear in the urine and the saliva. • Reactivation can also lead to vertical transmission. It is also possible for people who have experienced primary infection to be reinfected with another or the same strain of CMV, this reinfection does not differ clinically from reactivation. • In developed countries with a high standard of hygiene, 40% of adolescents are infected and ultimately 70% of the population is infected. In developing countries, over 90% of people are ultimately infected. Dr.T.V.Rao MD
Prevention Simple hand washing with soap and water is effective in removing the virus from the hands. Dr.T.V.Rao MD
raise CMV awareness? Dr.T.V.Rao MD
Visit for more articles of interest on Infectious Diseases Dr.T.V.Rao MD
Programme Created By Dr.T.V.Rao MD for Medical and Paramedical Students in the Developing World • Email • doctortvrao@hotmail.com Dr.T.V.Rao MD