Acinetobacter baumannii
1.97k likes | 9.56k Views
Acinetobacter baumannii is an important emerging pathogen of global importance early diagnosis and optimal treatment can reduce morbidity and mortality in hospitals and community

Acinetobacter baumannii
E N D
Presentation Transcript
Acinetobacter baumanniian emerging infection Dr.T.V.Rao MD
Acinetobacter baumanniianEmerging Bacterial Infection • Acinetobacter baumannii is a ubiquitous pathogen capable of causing both community and health care–associated infections (HAIs), although HAI’s are the most common form. This organism has emerged recently as a major cause of HAI because of the extent of its antimicrobial resistance and its propensity to cause large, often multifacility, nosocomial outbreaks.
Acinetobacter a Emerging Multidrug Resistant Bacteria • Since the 1970s, the spread of multidrug-resistant (MDR) Acinetobacter strains among critically ill, hospitalized patients, and subsequent epidemics, have become an increasing cause of concern. Reports of community-acquired Acinetobacter infections have also increased over the past decade. A recent manifestation of MDR Acinetobacter that has attracted public attention is its association with infections in severely injured soldiers.
Background:Acinetobacter baumannii • Gram negative bacillus • Water and soil • Associated with biofilms, antibiotic resistance • Survives on inanimate surfaces for weeks • Not part of normal human flora • Infections and outbreaks • Intensive care unit and healthcare settings • Compromised immune systems and risk • Colonized and infected patients as point sources
Several species among the Acinetobacter • The genus Acinetobacter comprises 17 validly named and 14 unnamed (genomic) species. Some unrelated (genomic) species have common designations, while some other species seem to be congruent but have different names. A phenotypic species identification system has been described and a variety of genotypic methods has been explored and applied to investigate the diversity or phylogeny in the genus.
Acinetobacter - Motionless • The name, Acinetobacter, comes from the Latin word for "motionless," because they lack cilia or flagella with which to move. Most species are not significant sources of infection. However, one opportunistic species, Acinetobacter baumannii, is found primarily in hospitals and poses a risk to people who have supressed immunity: According to the CDC, A. baumannii causes 80% of all Acinetobacter infections
Acinetobacter baumanniiMorphology • Acinetobacter baumannii is a pleomorphic aerobic gram-negative bacillus, commonly isolated from the hospital environment and hospitalized patients.
Morphology is distinctive • Rod shaped during rapid growth and coccobacillary in the stationary phase. • Encapsulated (generally). • Nonmotile (although they may exhibit twitching motility). • Gram-negative organisms. Retention of crystal violet may result in incorrect identification as gram-positive cocci.
Other species are occasional pathogens • A. baumannii is the major species of Acinetobacter. Others occasional human pathogens include A. calcoaceticus, A. lwoffi, A. junii, A. johnsonii and A. baylyi.
Current importance as Emerging Pathogen • Emerging as important global, pan-resistant GNB Nosocomial pathogen. • Clearly pathogenic when recovered from blood and normally sterile body sites. • May cause Nosocomial epidemics from contaminated common sources, e.g., ventilation equipment, catheters, etc.
Biochemical Reactions • Oxidase negative (opposite to Neisseria spp. or Moraxella spp.) • Haemolytic • Indole negative. • Catalase positive.
Biochemical Reactions Acidify glucose (may enhance its ability to invade devitalized tissue). • Grow at 44° C. • Aerobic. • Acinetobacter spp have the ability to use various sources of nutrition which accounts for its growth on routine laboratory media. This also explains its survival as an environmental pathogen.
Colony Characters • Colonies are 1 to 2 mm, nonpigmented, domed, and muciod, with smooth to pitted surfaces. • They can't reduce nitrate or to grow anaerobically (different from Enterobacteriaceae).
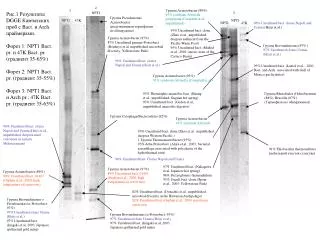
Newer methods of Identification of different species • Methods include high resolution fingerprinting with AFLP, PCR-RFLP with digestion of PCR amplified sequences, and analysis of various DNA sequences. Of these, AFLP analysis and amplified 16SrRNA ribosomal DNA restriction analysis have been validated with large numbers of strains of all described species. Nucleotide sequence based methods are expected to be the standard for identification in the near future.
Common species identified using • Acinetobacter calcoaceticus-baumanii complex: glucose-oxidising nonhemolytic, (A.baumannii can be identified by OXA-51 typing) • Acinetobacter lwoffii: glucose-negative nonhemolytic • Acinetobacter haemolyticus: haemolytic on blood agar.
Immune system and Acinetobacter Infections • Acinetobacter baumannii is a bacterium in the Acinetobacter genus which can be dangerous for human beings who have compromised immune systems, causing opportunistic infections which can lead to death if the patient does not receive aggressive treatment.
Survives in the natural environments with minimal needs • The organism can survive for months on clothing and bedclothes, bed rails, ventilators and other surfaces in the environment, including sinks and doorknobs, making Nosocomial transmission extremely difficult to control.
Transmission of: Acinetobacter • Transmission: Acinetobacter can be spread from person to person (infected or colonized patients), contact with contaminated surfaces of exposure to the environment.
Complex mechanisms of Drug Resitancemakes treatment options difficult
Documented mechanisms of resistance in Acinetobacter baumannii • Aminoglycosides-modifying enzymes • Broad-spectrum β-lactamases • Carbapenamases • Quantitative and/or qualitative changes in outer membrane porins • Altered penicillin-binding proteins.
Mechanisms for resistance to Carbapenems: • Metallo-β-lactamse (VIM, IMP): gene transfer, gene activation my insertion of an activation sequence (this is inserted upstream and switches on enzyme production) & mutation. • OXA Carbapenamases (class D) - difficult to detect. • Cell permeability changes. • Target (PBPs) change.
Emerging Mechanisms in Pathogenicty • A well-characterized porin of A. baumannii, the 38-kDa outer membrane protein A, has been shown to induce apoptosis of eukaryotic cells and to activate dendritic cells, leading to the differentiation of CD4+ T cells toward a Th1 phenotype
Biofilms enhance the Pathogenicty A. baumannii forms biofilms with enhanced antibiotic resistance and, more recently, that a chaperone-usher secretion system involved in Pilus assembly affects biofilm formation
what areMetallo-β-lactamses: • Common in the Far East, rare in Europe. • Various VIM & IMP types (plasmid mediated). • Extracts have been shown to hydrolyse imipenem. • High incidence in Pseudomonas aeruginosa referred to the HPA.
Iraqnobacter among US soldiers • Some nurses, soldiers, and microbiologists infected with Iraqnobacter (Acinetobacter baumanii) due to its spread throughout the military hospitals. Many times soldiers have survived hellacious trauma on the battlefield only to succumb to even more damage by an organism that has picked up antimicrobial resistance factors to the drugs primarily associated with treating them almost impossible.
Why it is important in critical care patients • Acinetobacter commonly colonizes patients in the intensive care setting. Acinetobacter colonization is particularly common in patients who are intubated and in those who have multiple intravenous lines or monitoring devices, surgical drains, or indwelling urinary catheters..
Hospitalized patients are highly venerable to Acinetobacter Infections • Acinetobacter infections are uncommon and occur almost exclusively in hospitalized patients
Co-humans ( HCW ) are great carriers of Infection • Acinetobacter causes colonization more often than infection; this means that it lives in or on the body without causing illness (e.g., the skin of a healthcare worker). People who are colonized can become carriers who spread the bacteria to other people, usually without realizing it.
Risk factors include: • hospitalization • significant co-morbidity • mechanical ventilation • cardio respiratory failure • previous infection • antimicrobial therapy • CVP lines • urinary catheters
Respiratory route is prominent route of entry • The respiratory system is the most common site for Acinetobacter infection because of its transient pharyngeal colonization of healthy persons and a high rate of tracheotomy colonization. Acinetobacter has been reported to cause community-acquired bronchiolitis and tracheobronchitis in healthy children.
Diagnosis of Acinetobacter Infections • Infection or colonization with Acinetobacter is usually diagnosed by clinical culture of blood, sputum, urine, wound, sterile body fluid, etc. Microbiologic cultures can be processed by standard methods on routine media.
Microbiological Investigation • Acinetobacter baumannii isolates were presumptively identified by using morphology of the colonies, Gram staining, Oxidase and Catalase reactions, growth at 44°C, and the API-20 NE System (Bio-Merieux, Lyon, France) Identification as A. baumannii was verified by restriction analysis of the 16S-23S ribosomal RNA intergenic-spacer sequences, (described by Dolzani and colleagues)
Problems in treatingAcinetobacter baumannii • One of the biggest issues with treating Acinetobacter baumannii is that the bacterium is naturally resistant to a number of antibiotics, making it challenging to find a drug regimen which will effectively attack it in an infected patien
Collect the following Data before decisions on Treatment • The following information will be collected: age, sex, occupation, hospital location at the time of positive culture (ER, medical ward, ICU etc), date of positive culture, prior hospitalization, receipt of outpatient dialysis, home care or other regular medical care (eg, outpatient chemotherapy), presence of invasive devices, receipt of antibiotics,
ICU’s – A potential source of Acinetobacter Infections • The elucidation of potential risk factors for resistant strains of Acinetobacter is therefore an important task, and the use of alternative antibiotics should be considered in ICUs where these strains are endemic .
Current trends in Antibiograms • Most A. baumannii are now resistant tampicillin, Carbencillin, Cefotaxime and Chloramphenicol. • Resistance to Gentamycin, tobramycin and amikacin is increasing. Flouroquinolones, ceftazidime, • Trimethoprim-Sulphmethoxazole, Doxycycline, Polymyxin B, colistin, imipenem and meropenem may retain activity against Nosocomial Acinetobacter
Treatment • Carbapenems (Imipenem and Meropenem) are the mainstay of treatment for antimicrobial-resistant gram-negative infections, though Carbapenems-resistant Acinetobacter is increasingly reported. • Resistance to the Carbapenems class of antibiotics makes multidrug-resistant Acinetobacter infections difficult, if not impossible, to treat.
Multidrug Resistant strains a Global Concern • Multidrug-resistant A. baumannii is a common problem in many hospitals in the US and Europe. First line treatment is with a Carbapenems antibiotic such as imipenem, but carbapenem resistance is increasingly common. Other treatment options include Polymyxin, tigecycline and Aminoglycosides.
Treating the Resistant Infections • Colistin and Polymyxin B have been used to treat highly resistant Acinetobacter infections. The choice of appropriate therapy is further complicated by the toxicity of colistin which is mainly renal. Acinetobacter isolates resistant to colistin and Polymyxin B have also been reported.
Medical interventions increasing the Acinetobacter Infections • Underlying diseases and severity of illness, presence of urinary or intravascular devices, recent immunomodulative therapies or radiation therapy, physical exam findings, laboratory and radiographical data, antimicrobial usage within 30 days of onset of the infection,
From Vietnam to Iraq • Recently A. baumannii has also been seen in a number of wound infections in soldiers returning from the middle east. Wound infections in soldiers is not a new phenomenon for A. baumannii as it was the most common gram negative bacillus to contaminate wounds during the Vietnam war as well.
Acinetobacter baumannii Infections in Iraq war • Since Operation Iraqi Freedom began in 2003, more than 700 US soldiers have been infected or colonized with Acinetobacter baumannii. A significant number of additional cases have been found in the Canadian and British armed forces, and among wounded Iraqi civilians.
Origin of Iraqibacter • Where the Iraqibacter came from remains something of a mystery. Soil samples taken by researchers in Iraq and Kuwait came back negative. However, it was found thriving in the hospitals. When Iraqibacter was compared to MDRAB samples taken in Europe before the war, they were found to be identical (Silberman, 2007). Thus, scientists believe that the current outbreak originated from European sources. ( So MDRAB did exist before the Iraq War.)
Can Acinetobacter Infect Health care Workers? • Acinetobacter rarely causes serious infection in otherwise healthy people and therefore poses minimal threat to healthcare workers or patients’ family members. • Pregnant healthcare workers are not at increased risk from this organism and can therefore care for patients infected or colonized with the organism.
Why Dealing with A.baumani infections is problematic. • A. baumannii important cause of nosocomial infections, in ICUs (Clin Microbiol Infect 2004;10:684—704) • Treatment difficult because multi-resistant • Colonized, infected patients point- sources of A. baumannii infections in healthcare settings • Prolonged organism survival on environmental surfaces in hospitals contributes to protracted outbreaks
Active surveillance of cultures • -Ventilator dependent /tracheotomy patients • -Patients admitted from long term care facilities with endemic Acinetobacter • -Patients with previous history of Acinetobacter infection
![MCM-41 loaded with [Mn(PaPy 3 )(NO)] + for the treatment of Acinetobacter baumannii](https://cdn2.slideserve.com/4562353/slide1-dt.jpg)